Definition
• DCO is a staged surgical strategy for musculoskeletal injuries in physiologically compromised polytrauma patients
• Principle: rapid temporary skeletal stabilisation → ICU resuscitation → delayed definitive fixation
• Philosophy: "Patient first, fracture second" — avoid iatrogenic "second hit" [1].
Physiological Rationale
First Hit / Second Hit Model
• First Hit: Initial trauma → massive tissue injury, haemorrhage, SIRS activation, DAMPs release
• Second Hit: Subsequent major stressor (e.g., lengthy definitive surgery) amplifies primed inflammatory cascade → ARDS, MODS, death
• DCO Role: DCO minimises surgical "second hit" → inflammatory response subsides before definitive fixation [2]
The Lethal Triad
• Hypothermia: Environmental exposure + cold fluids → impaired coagulation cascade enzymes
• Acidosis: Anaerobic metabolism from hypoperfusion → lactic acid ↑ → impaired cardiac & clotting function
• Coagulopathy: Factor consumption + dilution + inhibition by acidosis/hypothermia → uncontrolled bleeding
• Expanded to "Four Pathogenetic Cycles" with addition of Soft Tissue Injury → DAMPs → systemic inflammation [2]
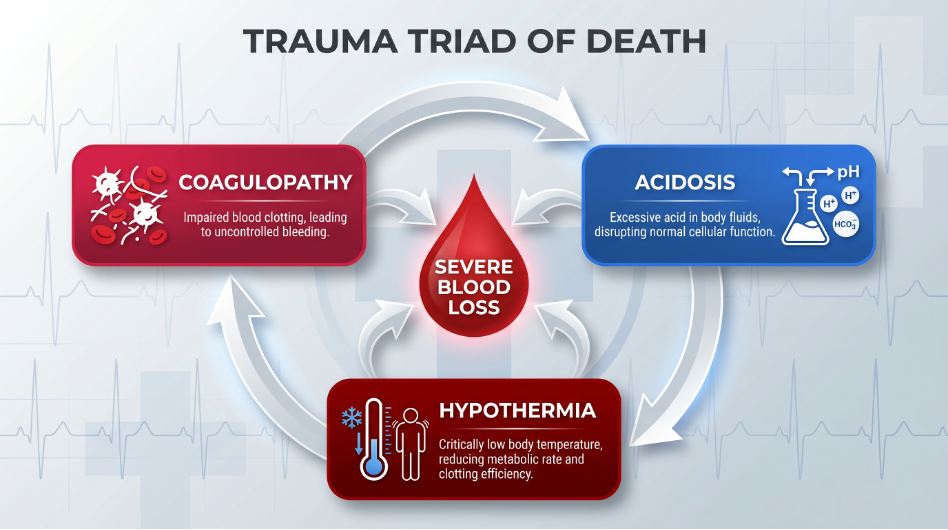
Figure 1. The Lethal Triad — hypothermia, acidosis, and coagulopathy form a self-perpetuating cycle.
Indications for DCO
• Unstable: Persistent haemodynamic instability (SBP < 90 mmHg despite resuscitation)
• Lethal triad present: core temp < 35°C, BE < −6.0, INR > 1.4
• Elevated lactate / poor clearance → ongoing shock; massive transfusion (> 10 units pRBCs)
• Borderline: ISS > 25–40, severe TBI (GCS < 8), bilateral pulmonary contusions, complex pelvic injuries
• Logistical: Mass casualty incidents; lack of specialised resources [3]
Contraindications (= Indications for ETC)
• Haemodynamically stable, no shock/coagulopathy, ISS < 16–20, isolated fractures[4]
Patient Categories
• Stable → Early Total Care appropriate
• Borderline → Clinical judgement; serial physiological monitoring
• Unstable → DCO indicated; temporary stabilisation only
• In Extremis → Abbreviated life-saving surgery only
DCO Staged Management
Stage 1: Acute Stabilisation (Day 0) [5]
• ATLS protocols → control haemorrhage (packing, angioembolisation)
• External fixation = workhorse of DCO: quick, minimally invasive, respects soft tissues
• Restores bone length/alignment → reduces pain, bleeding, inflammatory mediator release
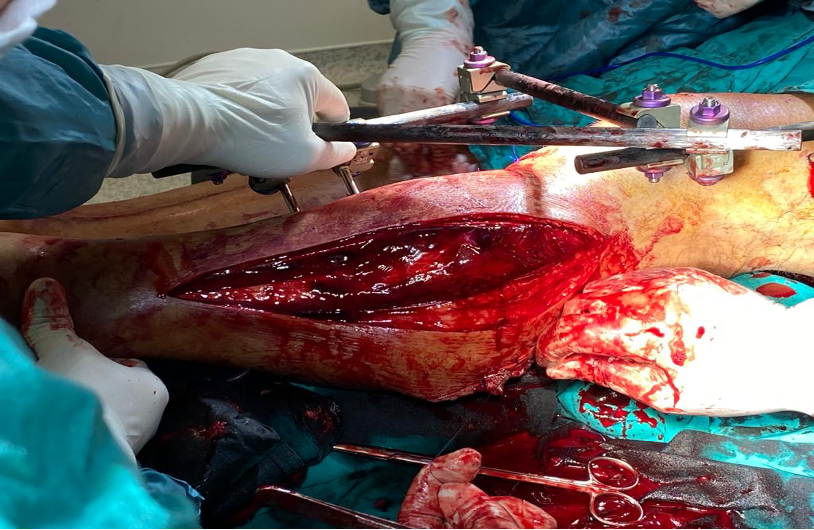
Figure 2. External fixation — cornerstone of Stage 1 DCO for rapid skeletal stabilisation.
Stage 2: ICU Resuscitation (Days 1–5)
• Aggressive warming, acidosis correction (lactate clearance), coagulopathy reversal
• Ventilatory support; daily trajectory assessment → platelet count, lactate, oxygenation [6]
Stage 3: Definitive Fixation (Condition-Based)
• Key: Timing is condition-based, NOT time-based → "Safe Definitive Surgery" (SDS) principle
• Readiness: lactate < 2.0–2.5 mmol/L, resolving coagulopathy, stable haemodynamics
• Convert external fixation → intramedullary nailing, plate/screw fixation as appropriate [7]
Clinical Decision-Making
Clinical Scenario | Decision | Action |
ISS < 20, stable | ETC | Definitive fixation |
ISS 20–40, borderline | Monitor | DCO if deteriorating; ETC if improving |
ISS > 40 / lethal triad | DCO | External fixation → ICU → staged definitive |
Severe TBI (GCS < 8) + fracture | DCO | Minimise operative time; avoid ICP ↑ |
Bilateral femur fractures | DCO | External fixation → staged nailing |
In extremis (pH < 7.1) | Abbreviated | Life-saving haemorrhage control only |
DCO vs Early Total Care (ETC)
Feature | DCO | ETC |
Philosophy | "Patient first, fracture second" | "Fix the fracture, fix the patient" |
Target | Unstable / borderline / polytrauma | Stable, isolated injuries |
Timing | Staged: temp fix → ICU → definitive | Immediate definitive (< 24h) |
Advantages | Reduces 2nd hit, ARDS/MOF risk | Shorter stay, less DVT/PE |
Disadvantages | Two procedures, pin-tract infection | High 2nd hit risk if misapplied |
Monitoring & Complications
• Key Parameters: Lactate + clearance (< 2.0), BE (> −6.0), core temp (> 36°C), INR/PT/aPTT, platelets (> 100 × 10⁹/L)
• ROTEM/TEG for real-time coagulation; IL-6 where available; urine output > 0.5 mL/kg/h
• Complications: Pin-tract infection, DVT/PE, malunion, ARDS/MOF, fat embolism, compartment syndrome [8]
Evolving Concepts
• Safe Definitive Surgery (SDS): Dynamic synthesis of DCO + ETC → repeated physiological assessment for optimal timing
• Early Appropriate Care (EAC): Physiology-guided timing and extent of surgery
• Rigid DCO vs ETC dichotomy → replaced by individualised, physiology-driven care
• Serial lactate clearance is more predictive than single admission values [9]
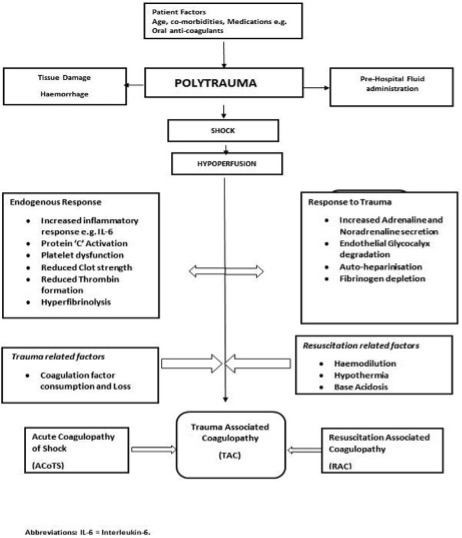
Figure 3. Polytrauma management algorithm — evolving decision-making concepts.
Pearls & Pitfalls
Pearls
✓ Physiology > fracture pattern — always base decisions on physiological status
• When in doubt with borderline patients → choose DCO
• External fixation is not failure — it is a deliberate, evidence-based, life-saving strategy
• DCO attenuates trauma-induced coagulopathy
• "Safe Definitive Surgery" replaces rigid time windows → operate when patient is ready
Pitfalls
✗ Applying ETC to an unstable/borderline patient → ARDS, MOF, death
• Delaying definitive fixation unnecessarily → malunion, DVT, prolonged immobilisation
• Ignoring the lethal triad before surgery; treating DCO as rigid protocol, not dynamic strategy
• Selection bias in studies → worse DCO outcomes often reflect higher initial injury severity
References
1. Roberts, C.S., et al., Damage control orthopaedics: evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr Course Lect, 2005. 54: p. 447–62.
2. Brohi, K., et al., Acute traumatic coagulopathy. J Trauma, 2003. 54(6): p. 1127–30.
3. Stahel, P.F., W.R. Smith, and E.E. Moore, Current trends in resuscitation strategy for the multiply injured patient. Injury, 2009. 40 Suppl 4: p. S27–35.
4. Giannoudi, M. and P. Harwood, Damage control resuscitation: lessons learned. Eur J Trauma Emerg Surg, 2016. 42(3): p. 273–82.
5. Giannoudis, V.P., et al., Severely injured patients: modern management strategies. EFORT Open Rev, 2023. 8(5): p. 382–396.
6. Pape, H.C. and L. Leenen, Polytrauma management - What is new and what is true in 2020 ? J Clin Orthop Trauma, 2021. 12(1): p. 88–95.
7. Rajasekaran, S., Updates and best practices in polytrauma. J Clin Orthop Trauma, 2021. 12(1): p. 8.
8. Pape, H.C., et al., The definition of polytrauma revisited: An international consensus process and proposal of the new 'Berlin definition'. J Trauma Acute Care Surg, 2014. 77(5): p. 780–786.
9. Van Ditshuizen, J.C., et al., The definition of major trauma using different revisions of the abbreviated injury scale. Scand J Trauma Resusc Emerg Med, 2021. 29(1): p. 71.