Overview
· Pediatric both-bone forearm fractures are injuries that directly compromise forearm rotational mechanics during childhood, with functional outcomes that are highly dependent on the accuracy and maintenance of anatomic reduction.
Epidemiology
· Forearm fractures account for approximately 18% of all fractures in the pediatric age group, and in about half of the cases, both bones are fractured concurrently.
· A male predominance is observed, with an approximate ratio of 2:1.
· The incidence increases during school age and adolescence.
Anatomy and Pathophysiology
· The forearm should be regarded as a functional unit rather than two independent long bones. Normal forearm function relies on coordinated motion between the radius and ulna, stabilized by the interosseous membrane and the proximal and distal radioulnar joints.
· The physiological radial bow is essential for forearm pronation–supination, and its malalignment or inadequate restoration can lead to permanent rotational loss.
· Remodeling capacity decreases with increasing age, thereby narrowing the limits of acceptable deformity.
· The distal radius accounts for approximately 75% and the distal ulna for approximately 81% of longitudinal forearm growth.
· In diaphyseal fractures, treatment tolerance increases from proximal to distal.
· Interosseous membrane tension:
· Neutral position and pronation → higher tension proximally
· Supination → higher tension distally
· Deforming muscular forces critical in both-bone forearm fractures: (Figure 1.)
· Proximal third:
· Biceps brachii and supinator → proximal fragment flexion and supination
· Middle third:
· Pronator quadratus pulls the distal fragment into pronation
· Pronator teres counterbalances the biceps effect → proximal fragment remains neutral
· Distal third:
· Brachioradialis → distal fragment dorsiflexion and radial deviation
· The injury most commonly results from a fall on an outstretched hand (FOOSH) combined with a rotational force.
· Anterior interosseous nerve (AIN) injury is the most frequently encountered nerve injury.
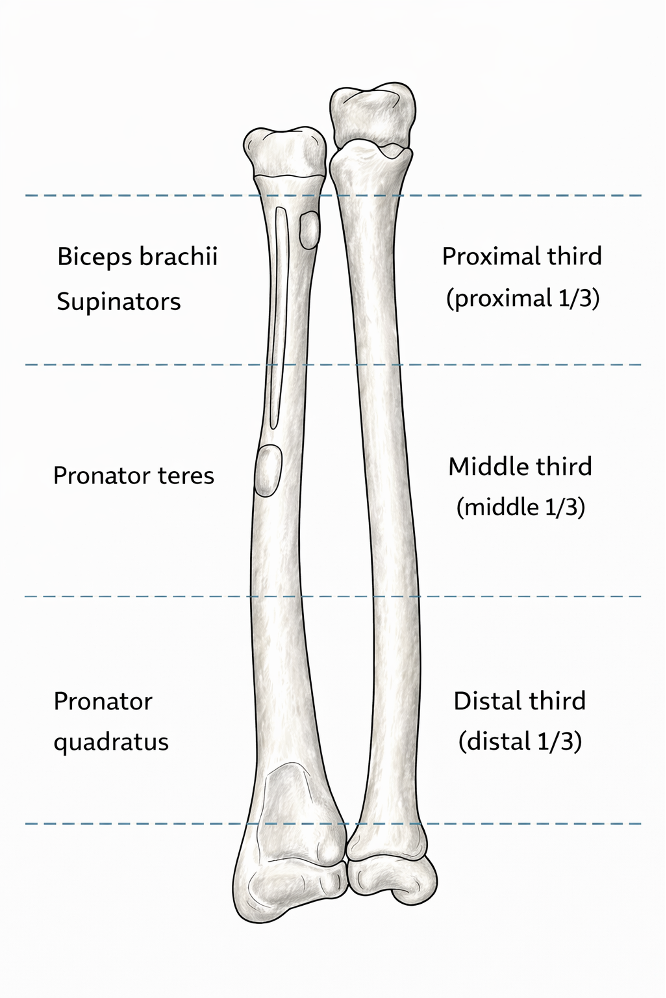
Figure 1. Forearm muscles and their insertion sites
Classification
· Classification according to anatomical location:
· Proximal
· Middle (midshaft)
· Distal
· Classification according to fracture pattern (Figure 2.)
· Incomplete
· Plastic deformation
· Torus
· Greenstick
· Complete and segmental fractures.

Figure 2. 1. Plastic deformation 2. Torus fracture 3. Greenstick fracture
Clinical Presentation
· Patients most commonly present with the following complaints after a fall.:
· Pain
· Deformity
· Limitation of forearm rotation
· Swelling
· Physical Examination
· The possibility of abuse in children under the age of 3 must always be kept in mind.
· A thorough neurovascular assessment is mandatory:
· Distal pulses
· Capillary refill
· Adjacent joints must be carefully examined:
· Elbow → Monteggia
· Wrist→ Galeazzi
Imaging
· Evaluation should be performed using anteroposterior (AP) and lateral radiographs of the entire forearm, including both the elbow and the wrist.
· Particular attention should be paid to measuring sagittal angulation of the radius on the lateral view.
· Normal radiographic alignment:
· AP view:
· The radial styloid is positioned 180° opposite the biceps tuberosity, with the biceps tuberosity oriented toward the ulnar side.
· Lateral view:
· The ulnar styloid is posterior and the coronoid process is anterior.
· The radial styloid and the biceps tuberosity are not visualized.
Treatment Principles
· Treatment decisions should be based on the patient’s age, fracture location, and the degree of residual deformity following reduction.
· The Noonan and Price criteria are still widely used; however, additional high-quality studies are required.
· Ploegmakers and colleagues evaluated acceptable deformity parameters across broader pediatric age groups. (Figure 3.)
Age Group | Acceptable Angulation | Acceptable Malrotation | Shortening |
< 5 years | ≤18° | ≤45° | <1 cm |
5–9 years | ≤15° | ≤45° | <1 cm |
9–12 years | ≤10°-8° | ≤30° | 0 |
≥12 years | 0 | 0 | 0 |
Figure 3. Acceptable deformity parameters based on Noonan-Pirce and Ploegmakers
Nonoperative Management
· Reduction Maneuvers
· Plastic deformation and greenstick fractures
· The deformity is corrected by applying gentle force in the direction opposite to the deformity, followed by cast application using the three-point molding principle. (Figure 4 and 5)
· Complete both-bone forearm fractures
· Initial management includes direct manipulation and finger-trap traction.
· In the presence of bayonet apposition, sustained longitudinal traction for 10–15 minutes may be attempted.
· Deformity is deliberately exaggerated to neutralize the deforming muscle forces, thereby ensuring that the broken fragments are aligned end-to-end. The deformity is then carefully corrected without loss of contact.
· If end-to-end contact cannot be achieved, bayonet apposition is considered acceptable provided angulation and rotational deformity remain within established limits.
· Casting
· Long-arm cast
· Elbow positioned at 90° of flexion
· Midshaft fractures: neutral or slight supination
· Pronation is rarely indicated
· Interosseous molding (anteroposterior compression)
· Medial and lateral molding over the humeral condyles
· Distal-third fractures
· No significant difference between pronation, supination, or neutral positioning
· Primary determinants are the quality of reduction and adequacy of cast molding
· Follow-up
· Early follow-up at 1–2 weeks
· Cast duration for stable alignment: 6–8 weeks
· Contact sports restricted for 4–6 months
· Outcomes
· Union rates approaching 100%
· Mean time to union: 6–10 weeks
· Residual angulation is common
· Functional pronation–supination is generally preserved
· Limitations in activities of daily living are rare
· Good functional outcomes reported with bayonet apposition
· No evidence demonstrating superiority over surgical treatment
· Complications
· Loss of reduction (8–14%)
· Cast index < 0.8 better outcomes (Figure 4.)
· Residual angulation
· Transient neuropraxia (median, ulnar, posterior interosseous nerve)
· Refracture, particularly within the first 6 months
· Rare: compartment syndrome
· Very rare: radioulnar synostosis

Figure 4. Three point molding and Cast index
Surgical Techniques
Open reduction internal fixation
· Technique
· Henry approach for the radius
· Subcutaneous ulnar approach for the ulna
· Limited periosteal stripping whenever possible
· Anatomic reduction
· Restoration of the radial bow (location and magnitude)
· Application of the compression principle
· DCP or LCP constructs
· Classic three-cortex screw fixation proximally and distally
ESIN (Elastic Stable Intramedullary Nailing; IMF)
· Technique
· Distal radial entry (lateral or dorsolateral variants), proximal to the physis
· Proximal ulnar entry through the olecranon region
· Nail diameter selection approximately 60% of the medullary canal or 2 mm smaller than the canal diameter
· Pre-bending of the radial nail according to the three-point contact principle
· Closed manipulation under fluoroscopic guidance
· Entry-point management with burying or trimming of the nail ends to minimize irritation
Outcomes
· Union rates and functional outcomes
· Comparable across all fixation methods
· Restoration of the radial bow
· Superior with plate fixation
· Tourniquet time, operative time, length of hospital stay, and cosmetic outcomes
· More favorable with ESIN
· Duration of immobilization and control of radial bowing
· More favorable with plate fixation
· Complications
· Risk of refracture after implant removal
· Higher with plate fixation
· Infection rates
· Comparable across all fixation methods
· Symptomatic implant prominence
· Extensor pollicis longus (EPL) tendon rupture, and superficial radial nerve injury
· ESIN constructs: implant removal typically recommended at approximately 6 months
· Early implant removal
· More frequently required after ESIN
Reference:
1. Shaw KA, Jamnik A, Shiver L, Kronenberger K, Harris H, Burks R, et al. Acceptable angulation criteria in pediatric midshaft forearm fractures: A systematic review and meta-analysis. J Pediatr Orthop Soc N Am. 2024 Feb;6:100013.
2. Ploegmakers JJW, Verheyen CCPM. Acceptance of angulation in the non-operative treatment of paediatric forearm fractures. J Pediatr Orthop B. 2006 Nov;15(6):428–32.
3. Mmerem K, Beeharry MW. Clinical and Radiological Outcomes of Paediatric Forearm Fractures of the Radius and Ulna Following Fixation by Intramedullary Nailing or Plating: A Systematic Review. Cureus [Internet]. 2023 Aug 16 [cited 2025 Dec 31];
4. Zionts LE, Zalavras CG, Gerhardt MB. Closed Treatment of Displaced Diaphyseal Both-Bone Forearm Fractures in Older Children and Adolescents: J Pediatr Orthop. 2005 July;25(4):507–12.
5. Upasani VV, Li Y. Elastic Intramedullary Nailing of Pediatric Both-Bone Forearm Fractures. JBJS Essent Surg Tech. 2020;10(4):e19.00055.
6. Poutoglidou F, Metaxiotis D, Kazas C, Alvanos D, Mpeletsiotis A. Flexible intramedullary nailing in the treatment of forearm fractures in children and adolescents, a systematic review. J Orthop. 2020 July;20:125–30.
7. Noonan KJ, Price CT. Forearm and Distal Radius Fractures in Children: J Am Acad Orthop Surg. 1998 May;6(3):146–56.
8. Ahmed AM, Said E, Addosooki A, Attya HA, Awad AK, Ahmed EH, et al. Intramedullary versus plate fixation of both bone forearm fractures in skeletally immature patients: a systematic review and meta-analysis. Eur J Orthop Surg Traumatol. 2024 Apr 20;34(5):2263–78.
9. Caruso G, Caldari E, Sturla FD, Caldaria A, Re DL, Pagetti P, et al. Management of pediatric forearm fractures: what is the best therapeutic choice? A narrative review of the literature. Musculoskelet Surg. 2021 Dec;105(3):225–34.
10. Boyer BA, Overton B, Schrader W, Riley P, Fleissner P. Position of Immobilization for Pediatric Forearm Fractures: J Pediatr Orthop. 2002 Mar;22(2):185–7.
11. Sharma O, Hamidi D, Bozzo I, Alrajhi K, Bernstein M. Surgical and Conservative Management are Both Effective for Pediatric Both Bone Forearm Fractures: A Systematic Review and Meta-Analysis. J Pediatr Orthop Soc N Am. 2025 Nov;13:100267.
12. Joeris A, Lutz N, Blumenthal A, Slongo T, Audigé L. The AO Pediatric Comprehensive Classification of Long Bone Fractures (PCCF): Part I: Location and morphology of 2,292 upper extremity fractures in children and adolescents. Acta Orthop. 2017 Mar 4;88(2):123–8.