Overview
Epidemiology
● Tibial shaft fractures account for approximately 15% of all pediatric fractures.
● They represent the third most common long-bone fracture in children, following femoral and forearm fractures.
Mechanism of Injury
● Typically demonstrates a bimodal distribution.
● Low-energy torsional injuries are common in toddlers, often resulting in spiral fractures.
● High-energy direct trauma (e.g., sports injuries, motor vehicle accidents) is more frequent in adolescents and commonly produces transverse or comminuted fracture patterns.
Biology
● The thick pediatric periosteum limits fracture displacement and promotes rapid healing.
● As a result, nonoperative management is the standard of care for the majority of cases.
Clinical Presentation
History
● A history of trauma is usually evident.
● In toddlers, the only presenting sign may be a subtle limp.
Physical Examination
● Pain, swelling, and inability to bear weight are consistently present clinical findings.
Soft-Tissue Assessment
● Careful evaluation of the skin is mandatory to identify open fractures.
● Neurovascular examination must be performed and documented.
Compartment Syndrome
● Less common in children than in adults but must be considered in high-energy injuries.
● The earliest clinical sign is pain disproportionate to the injury, often accompanied by an increased requirement for analgesia.
Imaging
Plain Radiography
● Anteroposterior (AP) and lateral radiographs of the tibia are diagnostic.
Rule of Two Joints
● Radiographs must include both the knee and ankle joints to exclude associated injuries (e.g., Maisonneuve fracture).
Computed Tomography (CT)
● Rarely indicated for diaphyseal fractures.
● Considered when intra-articular extension into the proximal or distal tibia is suspected.
Classification
Descriptive Classification
● Based on fracture pattern: transverse, oblique, spiral, or comminuted.
● Based on anatomical location: proximal third, middle third, or distal third.
AO Pediatric Comprehensive Classification of Long Bone Fractures (AO PCCF)
● Tibia/fibula segment is coded as 42.
● 42-D: Diaphyseal fractures, further categorized as simple, wedge, or complex.
Treatment
Conservative Management (Gold Standard)
Indications
● Closed, isolated tibial shaft fractures with acceptable alignment.
Acceptable Alignment Criteria
● Varus/valgus angulation: < 10°.
● Procurvatum/recurvatum: < 10–20° (sagittal plane remodeling is robust).
● Shortening: < 10–20 mm (overgrowth of approximately 10–15 mm is common in children younger than 10 years).
● Rotation: Remodeling does not correct rotational deformity; acceptable limit is < 5° of internal or external rotation.
Technique
● Initial immobilization with a long-leg cast with the knee flexed 10–20° for 4–6 weeks.
● Transition to a patellar tendon–bearing (PTB) cast or walking boot as healing progresses.
Surgical Management
Indications
● Open fractures.
● Compartment syndrome.
● Floating knee injuries (ipsilateral femoral fracture).
● Inability to maintain acceptable reduction in a cast.
● Severe polytrauma.
Elastic Stable Intramedullary Nailing (ESIN/TENS)
● Treatment of choice for unstable fractures in school-aged children (approximately 5–12 years).
● Allows controlled micromotion, promoting callus formation.
Rigid Intramedullary Nailing
● Reserved for skeletally mature adolescents with closed physes and an adult-type medullary canal.
Submuscular Plating
● Useful for fractures extending into the proximal or distal metaphysis where intramedullary nails provide insufficient stability.
Prognosis
Overall Outcomes
● Generally excellent, with the majority of patients achieving full functional recovery.
● Nonoperative management is associated with high union rates in stable fracture patterns.
Time to Recovery
● Return to normal activities typically occurs within 6–12 weeks.
● Recovery time depends on patient age, fracture characteristics, and treatment modality.
Operative Treatment Considerations
● Required for unstable, open, or comminuted fractures.
● Although associated with higher complication rates, appropriately indicated surgical treatment yields satisfactory outcomes.
Long-Term Follow-Up
● Recommended, particularly in younger children, to detect late complications such as leg-length discrepancy and residual angular deformity.
● Follow-up should consider remaining growth potential and fracture location.
Complications
Leg-Length Discrepancy (LLD)
● Most commonly caused by post-traumatic hyperemia and growth stimulation, leading to overgrowth of the injured limb.
● Less frequently associated with physeal injury resulting in growth arrest and limb shortening.
● Usually minimal and clinically insignificant; discrepancies greater than 1–1.5 cm are uncommon and more likely in younger children.
Acute Compartment Syndrome
● Rare but potentially limb-threatening.
● Typically associated with high-energy mechanisms and significant soft-tissue swelling.
● Requires early diagnosis and prompt fasciotomy to prevent permanent neuromuscular damage.
Delayed Union and Nonunion
● Rare in the pediatric population.
● More likely following high-energy trauma, open fractures, severe soft-tissue injury, or inadequate fracture stability.
● Operative stabilization (e.g., elastic stable intramedullary nailing) may reduce risk in selected cases.
Malunion and Angular Deformity
● One of the most common complications, particularly in distal diaphyseal fractures or cases with inadequate reduction and immobilization.
● Mild angular deformities often remodel due to the high remodeling potential of the pediatric tibia.
● Clinically significant malalignment may persist in older children and adolescents nearing skeletal maturity, potentially resulting in functional impairment.
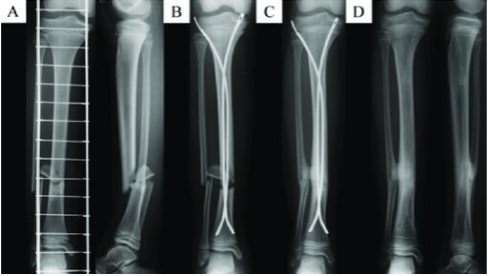
A 10-year-old girl with closed tibial shaft fracture (AO classification: 42D/4.2). (A) Preoperative anteroposterior and lateral radiographs. (B) Immediately postoperative anteroposterior radiographs. (C) 6 months after surgery, tibiofibular synostosis was detected with union. (D) Anteroposterior radiographs 14 months after surgery.

Figs. 1-A through 1-D Radiographs of a 4-year-old girl who had sustained a short spiral tibial shaft fracture while skiing.
Figs. 1-A and 1-B The patient was treated with gentle closed reduction and long leg cast immobilization.
Figs. 1-C and 1-D The patient subsequently progressed to healing in anatomic alignment.
References
1.AO Foundation. (2024). Pediatric tibia, diaphysis: Diagnosis and management. AO Surgery Reference. https://surgeryreference.aofoundation.org
2.Raducha JE, Swarup I, Schachne JM, Cruz AI Jr, Fabricant PD. Tibial Shaft Fractures in Children and Adolescents. JBJS Rev. 2019 Feb;7(2):e4. doi: 10.2106/JBJS.RVW.18.00047. PMID: 30817691.
3.Waters PM, Skaggs DL, Flynn JM. Rockwood and Wilkins’ Fractures in Children. 9th ed. Philadelphia: Wolters Kluwer; 2019.
4.Bauer JM, Lovejoy SA. Toddler's Fractures: Time to Weight-bear With Regard to Immobilization Type and Radiographic Monitoring. J Pediatr Orthop. 2019 Jul;39(6):314-317. doi: 10.1097/BPO.0000000000000948. PMID: 31169752.
5.Maleki A, Qoreishy M, Kazemi S M, Yahya G. Pediatric Tibial Shaft Fractures Remodeling After Casting. JROS 2022; 9 (2) :93-98 URL: http://jros.iums.ac.ir/article-1-2204-en.html
6.Stenroos A, Puhakka J, Nietosvaara Y, Kosola J. Treatment of Closed Tibia Shaft Fractures in Children: A Systematic Review and Meta-Analysis. Eur J Pediatr Surg. 2020 Dec;30(6):483-489. doi: 10.1055/s-0039-1693991. Epub 2019 Aug 22. PMID: 31437858.
7.Cruz AI Jr, Raducha JE, Swarup I, Schachne JM, Fabricant PD. Evidence-based update on the surgical treatment of pediatric tibial shaft fractures. Curr Opin Pediatr. 2019 Feb;31(1):92-102. doi: 10.1097/MOP.0000000000000704. PMID: 30461511.
8.Miyamoto, S.; Otsuka, M.; Hasue, F.; Fujiyoshi, T.; Kamiya, K.; Kiuchi, H.; Odagiri, T.; Tanaka, T.; Nakamura, J.; Orita, S.; Ohtori, S. Associated Injury Complicated by Pediatric Lower Limb Shaft Fractures and Clinical Efficacy of Flexible Stainless-Steel Intramedullary Nailing in Children Less than 15 Years Old. Orthopedic Reviews 2021, 13. https://doi.org/10.4081/or.2021.8008.
9.Raducha, J.; Swarup, I.; Schachne, J.; Cruz, A.; Fabricant, P. Tibial Shaft Fractures in Children and Adolescents. JBJS Reviews 2019, 7, 1. https://doi.org/10.2106/JBJS.RVW.18.00047.