Physical Exam Components
Inspection – Palpation – Range of Motion (ROM) – Strength – Neurovascular Examination – Stability – Special Tests
General Principles
Always perform a side-to-side comparison.
Examine the elbow in a stepwise and reproducible sequence.
Differentiate pain-limited motion from true mechanical restriction.
Small ROM losses at the elbow may have significant functional impact.
Correlate physical findings with pain location and activity-related symptoms.
1) Inspection
Inspect with the patient seated or standing, arms relaxed.
Skin
Surgical scars, abrasions, erythema
Ecchymosis (acute trauma)
Skin atrophy or color changes (chronic neuropathy/CRPS)
Swelling
Posterior swelling over the olecranon (bursitis)
Diffuse swelling (effusion, inflammatory arthritis)
Alignment
Carrying angle (normally 10–15° valgus)
Cubitus valgus or varus deformity
Muscle bulk
Forearm or arm atrophy (chronic nerve injury or disuse)
Dynamic observation
Snapping during flexion–extension (ulnar nerve, snapping triceps)
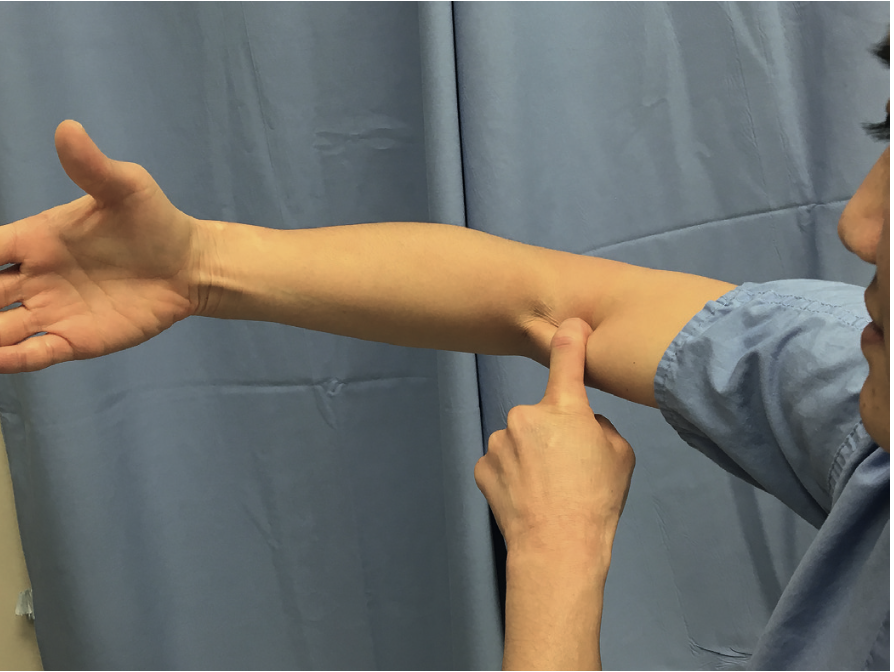
2) Palpation
A) Anterior Compartment
Palpate structures from lateral to medial:
Radial nerve
Distal biceps tendon
Brachial artery
Median nerve
Distal biceps
Tenderness, gap, or asymmetry
Hook test to assess tendon continuity
B) Lateral Compartment
Lateral epicondyle
Point tenderness suggests lateral epicondylitis
Radial head
Palpate during pronation–supination
Pain suggests radiocapitellar pathology
Radial tunnel (≈4 cm distal to epicondyle)
C) Medial Compartment
Medial epicondyle
Cubital tunnel
Ulnar nerve tenderness, thickening, or subluxation
Flexor–pronator mass origin
D) Posterior Compartment
Olecranon
Bursal thickening, warmth, fluctuation
Triceps insertion
Posteromedial olecranon (valgus extension overload)
Clinical note
Localized tenderness combined with a provocative maneuver is highly suggestive of regional pathology.
3) Range of Motion (ROM)
A) Elbow Motion
Assess active and passive flexion–extension.
Normal range: 0–140°
Functional range: 30–130°
Loss of terminal extension is often the earliest abnormality.
B) Forearm Rotation
Elbow flexed to 90°, arm adducted.
Normal:
Pronation: 75–80°
Supination: 80–85°
Functional arc: 50° pronation + 50° supination
Observe for shoulder compensation.
Interpretation
Passive < active limitation → pain inhibition or weakness
Passive restriction → contracture, osteophytes, intra-articular pathology
4) Strength Examination
Test with elbow at 90° flexion.
Flexion: biceps, brachialis
Extension: triceps
Weak terminal extension → triceps injury
Pronation / Supination
Grip strength
Reflects global upper extremity function
5) Neurovascular Examination
Motor and sensory evaluation of:
Radial nerve (wrist/finger extension)
Median nerve (thumb opposition, sensation)
Ulnar nerve (finger abduction/adduction)
Vascular
Brachial and radial pulses
Mandatory documentation in trauma or instability cases
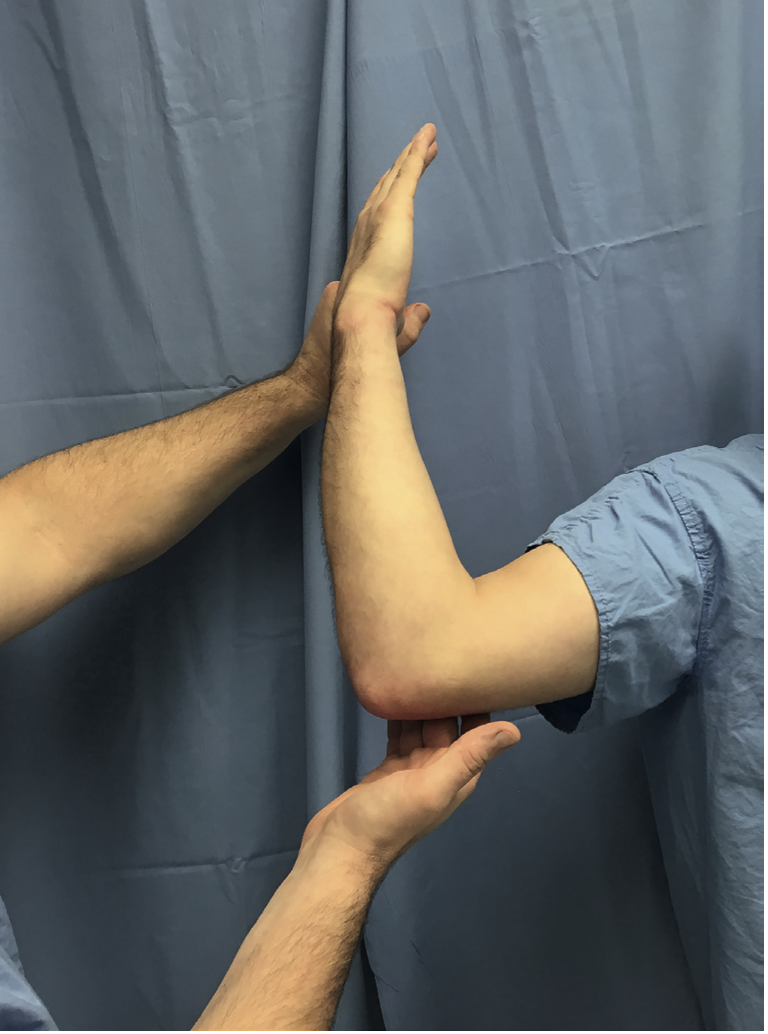
6) Stability Examination
A) Valgus Stability (MUCL)
Milking maneuver
Elbow ~90° flexion, valgus stress applied
Moving valgus stress test
Pain between 70–120° flexion is positive
Valgus extension overload
Posterior pain with extension + valgus stress
Common in overhead athletes
B) Varus Stability (LCL Complex)
Elbow slightly flexed (~15°)
Apply varus stress with forearm supinated
Excessive opening suggests LCL injury
C) Posterolateral Rotatory Instability (PLRI)
Pivot-shift test (often painful or apprehensive)
Posterolateral rotatory drawer
Chair push-up / push-up test
Apprehension or inability to perform indicates instability
D) Varus Posteromedial Rotatory Instability
Gravity-assisted varus grind test
Crepitus or pain suggests anteromedial coronoid involvement
7) Special Tests
Lateral Elbow
Resisted wrist extension
Pain at lateral epicondyle → lateral epicondylitis
Tennis Elbow Shear Test (TEST)
Resisted long-finger extension
Pain distal to epicondyle → radial tunnel syndrome
Medial Elbow
Resisted wrist flexion/pronation
Medial TEST
Face press test
Serving tray test
Suggests flexor–pronator pathology or MUCL involvement
Posterior Elbow
Posterior arm bar test
Pain → posterior impingement or osteophytes
Resisted extension → triceps pathology
Anterior Elbow
Hook test
Absence of tendon → distal biceps rupture
Radiocapitellar compression test
Pain with pronation + resisted extension
Key Clinical Pearls
A normal elbow ROM makes major intra-articular pathology unlikely.
Extension loss is the most sensitive ROM abnormality.
Mild contractures may be functionally tolerated.
Always integrate exam findings with mechanism of injury and activity demands.
References
• Morrey's The Elbow and Its Disorders, Fifth Edition