Introduction
Definition: A minimally invasive spine surgery (MISS) technique using high-definition endoscopes to treat spinal pathology through small (typically <1cm) incisions.
Core Philosophy: Minimal muscle dissection, preservation of the "posterior complex" (ligamentum flavum, multifidus), and direct visualization of neural structures.
Pre-operative Planning & Imaging
· Iliac Crest Assessment: Evaluate the height of the iliac crest on lateral radiographs, especially for L5-S1 transforaminal access. High crest may necessitate an interlaminar approach
· CT Scans: Indicated to identify facet hypertrophy, syndesmophytes, or calcified disc fragments that may require specialized endoscopic burrs.
· MRI Analysis: Detailed mapping of the "target zone" and assessment of the foraminal window size to plan the optimal entry point and trajectory.
Approaches
1. Transforaminal Approach
Indication: Far-lateral or foraminal disc herniations.
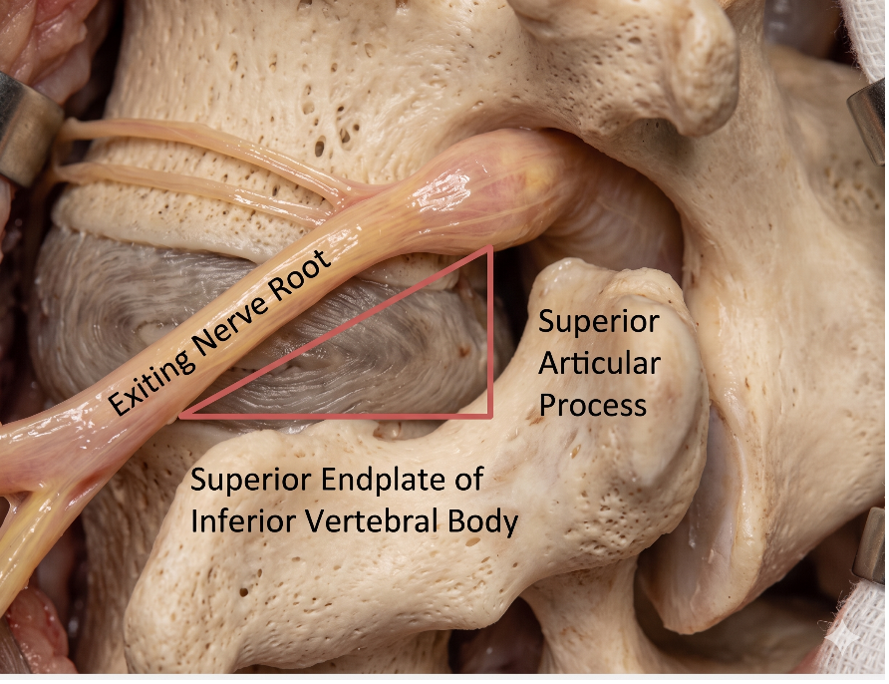
Technique: Access through Kambin’s Triangle.
Boundaries of Kambin’s Triangle:
Hypotenuse: Exiting nerve root.
Base: Superior border of the inferior vertebra.
Height: Traversing nerve root/thecal sac.
2. Interlaminar Approach
Indication: L5-S1 herniations (where the iliac crest blocks transforaminal access) or central canal stenosis.
Technique: Similar to a traditional microdiscectomy but using an endoscope and specialized shavers/burrs through the interlaminar window.
Indications
Lumbar Disc Herniation (LDH): The most common indication.
Spinal Stenosis: Lateral recess or central stenosis
Foraminal Stenosis: Foraminoplasty using endoscopic burrs.
Failed Back Surgery Syndrome (FBSS): Managing recurrent herniations through virgin tissue planes.
Equipment & Instrumentation
Endoscope: High-definition camera with a working channel (typically 2.5mm to 4.2mm).
Constant Irrigation: Saline flow maintains visualization, controls bleeding (hydrostatic pressure), and flushes debris.
Radiofrequency (RF) Ablation: Used for hemostasis and "shrinking" the annulotomy.
Procedure Steps (Lumbar Discectomy)
Localization: Fluoroscopic guidance to mark the entry point.
Dilation: Serial dilators to move muscle fibers without cutting.
Cannula Placement: The working sleeve is docked on the target (e.g., the lamina or the foramen).
Visualization: Identification of the ligamentum flavum, epidural fat, and the nerve root.
Discectomy: Removal of the herniated fragment using endoscopic graspers.
Verification: Confirming the "free-floating" nerve root.
Advantages vs. Traditional Microdiscectomy
Reduced "Approach-Related" Morbidity: Less muscle atrophy and postoperative pain.
Faster Recovery: Many procedures are performed in outpatient settings (same-day discharge).
Minimal Blood Loss: Due to constant irrigation and small incision.
Better Visualization: High-magnification and the ability to look "around the corner" with angled lenses.
Post-operative Care & Discharge
· Mobilization: Immediate mobilization is typically encouraged; most patients are ambulatory within 1-2 hours post-procedure.
· Orthosis: Lumbar bracing is generally not required, though a soft corset may be used for 2 weeks for patient comfort and proprioception.
· Return to Activity: Sedentary work can often be resumed within 1 week; gradual return to heavy labor or sports after 4-6 weeks.
Complications
Dural Tear: Difficult to repair endoscopically (often requires conversion or specialized sealants).
Nerve Root Injury: Risk of irritation to the exiting nerve root in the transforaminal approach.
Dysesthesia: Often transient, due to manipulation of the dorsal root ganglion (DRG).
Incomplete Decompression: Most common during the "learning curve" phase.
Pits & Pearls
Pearl: The "Learning Curve" is steep. It typically takes 20–30 cases to achieve proficiency comparable to open microdiscectomy.
Pitfall: Fluid Management. Ensure adequate outflow of irrigation to prevent increased epidural pressure or "neck pain" (in cervical cases) due to cephalad fluid migration. To avoid retinal damage, do not increase the washing fluid pressure above 50 mmHg.
Tip: Always use a "Beveled" cannula; it acts as a nerve root retractor and a protector for your instruments.