Figures
Definition
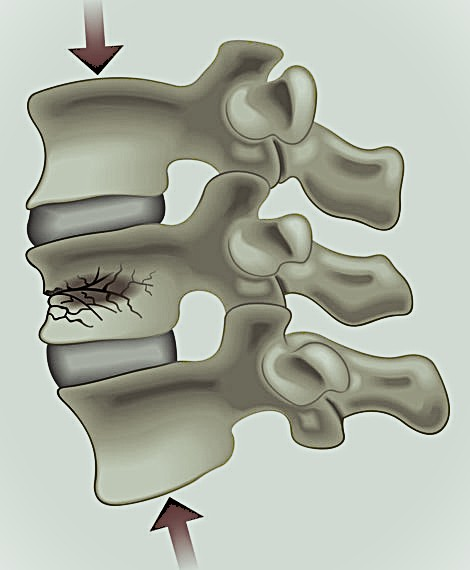
Collapse of the vertebral body, typically involving the anterior column
Results in loss of vertebral height without posterior wall disruption (in simple cases)
Most commonly affects the thoracolumbar junction (T12–L2)
Epidemiology
Common in:
Elderly patients (osteoporosis-related)
Postmenopausal women
Increasing incidence with age
Also seen in:
Trauma
Malignancy (pathological fractures)
Etiology / Risk Factors
Osteoporotic
Most common cause
Low-energy trauma (e.g., fall from standing height)
Traumatic
High-energy axial load
Usually in younger patients
Pathological
Metastases
Multiple myeloma
Primary bone tumours
Pathophysiology
Axial load → failure of anterior vertebral body
Leads to:
Wedge deformity
Increased kyphosis
Repeated fractures → sagittal imbalance
Classification
Genant Classification (Osteoporotic)
Grade 1 (Mild): 20–25% height loss
Grade 2 (Moderate): 25–40% height loss
Grade 3 (Severe): >40% height loss
AO Spine (Type A1)
Wedge compression fracture
No involvement of posterior wall
Typically stable
Clinical Presentation
Acute back pain (sudden onset)
Pain worsens with:
Standing
Movement
Improves with rest
Chronic cases:
Height loss
Kyphotic deformity (“dowager’s hump”)
Neurological deficit → uncommon (suggests alternative diagnosis)
Red Flags
Night pain
Unexplained weight loss
Neurological deficit
History of malignancy
Consider pathological fracture
Imaging
X-ray
First-line
Anterior wedge deformity
Loss of vertebral height
MRI
Distinguishes:
Acute vs chronic fracture
Benign vs malignant
Shows bone marrow oedema
CT
Detailed fracture anatomy
Useful if posterior wall involvement suspected
Diagnosis
Clinical + imaging
Always assess:
Stability
Neurological status
Underlying cause (osteoporosis vs malignancy)
Treatment
Nonoperative (First-line in most cases)
Indications:
Stable fracture
No neurological deficit
Management:
Analgesia
Early mobilisation
Bracing (TLSO – optional, controversial)
Osteoporosis treatment:
Calcium / Vitamin D
Bisphosphonates.
Interventional Procedures
Vertebroplasty
Cement injection into vertebral body
Rapid pain relief
Controversial efficacy
Kyphoplasty
Balloon expansion + cement
Restores some vertebral height
May reduce kyphosis
Consider in:
Persistent severe pain
Failure of conservative treatment
Operative Treatment
Rare, but indicated if:
Neurological deficit
Significant instability
Progressive deformity
Complications
Chronic pain
Progressive kyphosis
Adjacent level fractures
Reduced pulmonary function (severe kyphosis)
Prognosis
Most improve with conservative management
Recurrent fractures common in osteoporosis
Functional decline possible in elderly patients
Pits & Pearls
Most VCFs are osteoporotic and stable
Neurological deficit → think NOT simple compression fracture
MRI is key for:
Acute vs chronic
Malignancy suspicion
Treat the underlying osteoporosis, not just the fracture
Pitfalls
Missing pathological fracture (especially metastasis/myeloma)
Overusing vertebroplasty without clear indication
Ignoring osteoporosis management
Misinterpreting old fractures as acute
Not evaluating for multiple-level involvement
Management Algorithm (Compression Fractures: Conservative vs Kyphoplasty)
Step 1: Confirm Diagnosis
Imaging (X-ray ± MRI)
Identify:
Acute vs chronic fracture
Benign vs pathological
If malignancy suspected → biopsy / oncologic pathway
Step 2: Assess Stability & Neurology
Neurological deficit?
Yes → Surgical evaluation (not kyphoplasty)
No → proceed
Posterior wall involvement / instability?
Yes → consider surgical stabilisation
No → proceed
Step 3: Initial Conservative Management (First-line)
Indications:
Stable fracture
No neurological deficit
Treatment:
Analgesia
Early mobilisation
± TLSO brace
Osteoporosis management
Step 4: Reassess at 2–6 Weeks
Evaluate:
Pain level
Functional status
Ability to mobilise
Step 5: Decision Point
Continue Conservative Treatment
Pain improving
Functional recovery present
Mobilisation possible
Consider Kyphoplasty
Indications:
Persistent severe pain despite adequate conservative treatment
Pain limiting mobilisation / ADLs
MRI-confirmed acute fracture (bone marrow oedema)
No posterior wall compromise
Avoid Kyphoplasty
Asymptomatic or improving patient
Chronic fracture (no oedema on MRI)
Unstable fracture
Neurological deficit
Quick Flow Summary
Stable + improving → Conservative
Stable + persistent severe pain → Kyphoplasty
Instability or neuro deficit → Surgery (not kyphoplasty)
Clinical Pearls
Kyphoplasty is pain-driven, not imaging-driven alone
MRI oedema = key indicator of “treatable” acute fracture
Early mobilisation is critical → prolonged bed rest worsens outcomes
Always initiate osteoporosis treatment
Common Pitfalls
Performing kyphoplasty in chronic fractures
Ignoring posterior wall involvement
Over-treating mild, improving cases
Missing underlying malignancy
Delaying mobilisation unnecessarily