Overview
• Monteggia fracture is defined as a proximal one-third ulnar shaft fracture combined with radial head dislocation.
• First described by Monteggia et al. in 1814, later studies included olecranon fractures as part of this injury pattern.
• Represents <2% of all forearm injuries in both children and adults.
• Missed or delayed diagnosis can result in forearm deformity and dysfunction, leading to neglected Monteggia fracture (1).
• Complex variants may involve:
◦ Coronoid fracture with metaphyseal extension
◦ Proximal radius fracture
◦ Ulnohumeral instability (2)
Clinical Presentation
• Initial evaluation must assess:
◦ Skin integrity
◦ Neurovascular status
◦ Compartment pressures
• Posterior interosseous nerve palsy is the most common nerve injury associated with Monteggia fractures (2).
Classification (Bado Classification)
Bado described four types based on ulnar angulation and direction of radial head displacement (3):
• Type I: Apex anterior proximal ulna fracture + anterior radial head dislocation
→ Most common in pediatric population
• Type II: Apex posterior proximal ulna fracture + posterior radial head dislocation
→ Most common in adults
• Type III: Metaphyseal fracture of proximal ulna + lateral or anterolateral radial head dislocation
• Type IV: Anterior radial head dislocation + ipsilateral proximal radial shaft fracture
Imaging
• Standard views: Anteroposterior and lateral radiographs of the elbow, forearm, and wrist (Figure 1).
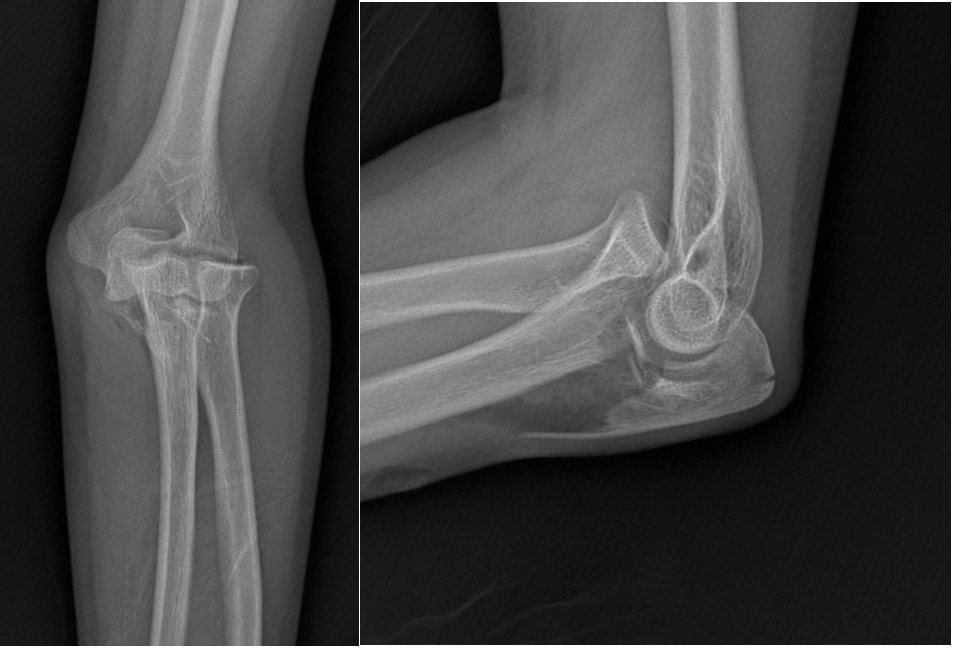
Figure 1
• Oblique radiographs may assist in further classification.
• CT scan is useful for:
◦ Preoperative planning
◦ Detecting subtle or chronic injuries
◦ Assessing nonunion (2)
Treatment
• In adults, open reduction and internal fixation (ORIF) of the ulna is the treatment of choice.
• May require:
◦ Fixation or replacement of the radial head
◦ Repair of lateral ligamentous structures, if necessary (3)
Surgical Indications
• Anatomic restoration of proximal ulna is critical for optimal outcomes.
• Following ulnar fixation, radiographic evaluation of radiocapitellar alignment is mandatory (Figure 2).
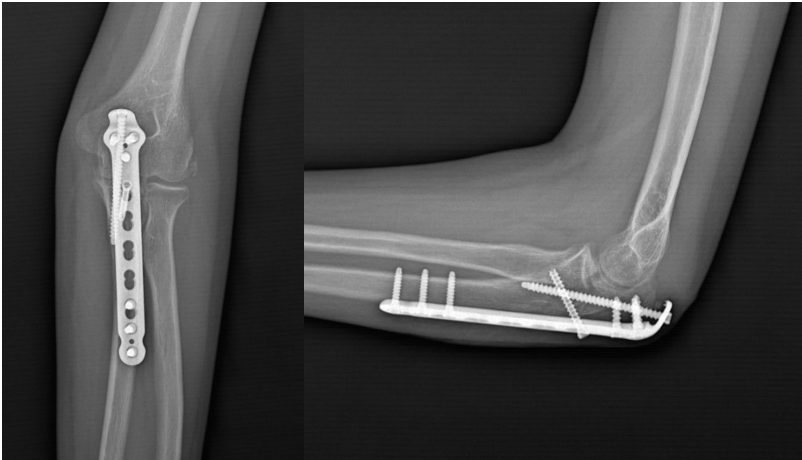
Figure 2
• Persistent dislocation/subluxation after ulnar reduction may indicate soft-tissue interposition (annular ligament, capsule, etc.), requiring removal through a separate lateral incision (3).
Prognosis
• Most common complication: Implant irritation due to soft-tissue contact (13,35).
• Other possible complications:
◦ Malunion / nonunion
◦ Nerve irritation
◦ Limited elbow range of motion
◦ Recurrent radial head dislocation
◦ Infection (2)
Differential Diagnosis
Conditions that may mimic Monteggia fracture (proximal ulna fracture with radial head dislocation) include (4):
• Isolated radial head dislocation
• Radial neck fracture
• Proximal ulna fracture without radial head dislocation
• Olecranon fracture
• Posterior or posterolateral elbow dislocation
• Forearm fractures without dislocation
• Monteggia-equivalent lesions
References
1- Zhang R, Wang X, Xu J, Kang Q, Hamdy RC. Neglected Monteggia fracture: a review. EFORT Open Rev. 2022 Apr 21;7(4):287-294. doi: 10.1530/EOR-21-0087. PMID: 35446261; PMCID: PMC9069855.
2- Soderlund T, Zipperstein J, Athwal GS, Hoekzema N. Monteggia Fracture Dislocation. J Orthop Trauma. 2024 Sep 1;38(9S):S26-S30. doi: 10.1097/BOT.0000000000002854. PMID: 39150291.
3- Patel M, Dehghan N. Management of Monteggia Injuries in the Adult. Hand Clin. 2020 Nov;36(4):479-484. doi: 10.1016/j.hcl.2020.07.002. Epub 2020 Sep 2. PMID: 33040960.
4- Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM. The management of Monteggia fractures. J Bone Joint Surg Am. 1991;73(2):219–224.