Overview
• The subcutaneous location of the ulna makes it susceptible to trauma and fractures.
• Fractures of the olecranon account for up to 40% of all fractures around the elbow joint (1).
• Most olecranon fractures occur due to:
◦ Direct impact of traumatic force from the distal humerus to the proximal ulna.
◦ Indirect traction by the triceps tendon pulling the proximal ulna.
Clinical Presentation
• Commonly caused by a direct blow onto the olecranon from a low-height fall or during forceful extension (2).
• The elbow is usually swollen with joint effusion.
• The superficial position of the olecranon allows easy palpation, making discontinuity or depression at the fracture site readily detectable.
Classification
• One of the most commonly used systems in clinical practice is the Mayo classification (Figure 1).
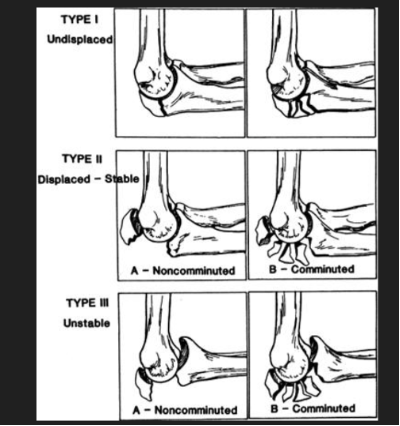
Figure 1
• Another classification system used is the Colton classification (Figure 2).
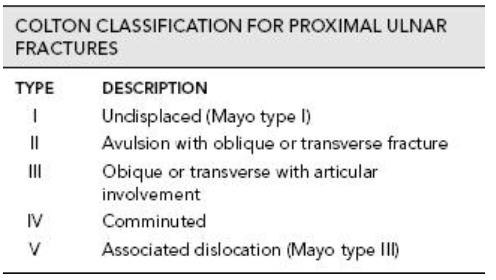
Figure 2
Imaging
• In simple fractures, standard anteroposterior and lateral elbow radiographs are usually sufficient. (Figure 3)
• Computed tomography is not routinely required for simple transverse olecranon fractures.
• It may, however, be helpful for preoperative planning in comminuted fracture patterns (3).

Figure 3
Treatment
• All olecranon fractures are intra-articular.
• Therefore, the goal of treatment—as defined by the AO group—is:
◦ Anatomic restoration of the articular surface.
◦ Stable fixation of the fracture.
◦ Early mobilization of the joint.
Surgical Indications
• Non-displaced fractures of the olecranon (Mayo Type IA and IB) may be treated conservatively.
• These are cases with less than 2 mm of displacement and no change in position when the elbow is gently flexed to 90° or fully extended against gravity.
• In conservative management:
◦ The elbow is immobilized at 45–90° flexion for 3–4 weeks.
◦ Flexion up to 90° is then initiated.
◦ Radiographic signs of union are expected by 6–8 weeks, after which motion is gradually increased (4).
• Surgical management is traditionally performed using:
◦ Tension band wiring, or
◦ Plate fixation.
• Both techniques can be performed with the patient in the lateral position, arm resting over a post, and using a sterile tourniquet for a bloodless field.
• A posterior skin incision is made over the olecranon, avoiding the bursa and ulnar nerve.
• Tension band wiring principle: converts the distracting force of the triceps into a compressive force to promote healing. (Figure 4)
• Surgical steps:
◦ Fracture reduction and temporary fixation with a clamp.
◦ Two parallel Kirschner wires passed from the olecranon tip across the fracture to the anterior cortex.
◦ Drill hole created distal to the fracture; cerclage wire passed in a figure-of-eight configuration and tightened.
◦ Wire ends cut short and buried; K-wires bent, cut, and sunk into triceps tendon.
• Open reduction and internal fixation (ORIF) with pre-contoured locking plates is more suitable for displaced comminuted (Mayo IIB) and unstable displaced (Mayo III)
fractures to achieve anatomic reduction (3).


Figure 4
Prognosis
• Karlsson et al. reported that 96% of patients treated with different techniques (conservative, TBW, figure-of-eight, or Rush pins) achieved excellent or good results, despite reduced range of motion and degenerative changes on follow-up radiographs (5).
• The most common postoperative complications:
◦ Pain and hardware prominence.
◦ K-wire migration requiring removal.
• Other reported complications:
◦ Loss of range of motion.
◦ Degenerative changes of the elbow joint.
◦ Nerve or vascular injuries.
◦ Nonunions, heterotopic ossification, and infection (1).
Differential Diagnosis
• Lesions with similar clinical and radiographic features should be considered (6):
◦ Posterior Monteggia lesion
◦ Triceps tendon rupture
◦ Olecranon apophyseal separation (children)
◦ Olecranon bursitis
References:
1- Schneider MM, Nowak TE, Bastian L, Katthagen JC, Isenberg J, Rommens PM, Müller LP, Burkhart KJ. Tension band wiring in olecranon fractures: the myth of technical simplicity and osteosynthetical perfection. Int Orthop. 2014 Apr;38(4):847-55. doi: 10.1007/s00264-013-2208-7. Epub 2013 Dec 12. PMID: 24326359; PMCID: PMC3971280.
2- Adams JE, Steinmann SP. Fracture of the olecranon. In: Morrey BF, Sanchez-Sotelo J, editor. The Elbow and Its Disorders. 4th edition. Philedelphia: Saunders, Elsevier; 2009. p.389–400.
3- (Karthikappallil D, Cash T, Fischer J, Waseem M. Olecranon fractures: applied anatomy, clinical assessment and evidence-based management. Br J Hosp Med (Lond). 2022 Feb 2;83(2):1-7. doi: 10.12968/hmed.2021.0272. Epub 2022 Feb 23. PMID: 35243890.)
4- (Hak DJ, Golladay GJ. Olecranon fractures: treatment options. J Am Acad Orthop Surg 2000;8(4):266–75.)
5- (Karlsson MK, Hasserius R, Karlsson C, Besjakov J, Josefsson PO. Fractures of the olecranon: a 15- to 25-year followup of 73 patients. Clin Orthop Relat Res. 2002 Oct;(403):205-12. PMID: 12360028.)
6- (Rockwood CA, Green DP, Bucholz RW, et al. Rockwood and Green’s Fractures in Adults. 9th ed. Philadelphia: Wolters Kluwer; 2020. p.1120–1138.)