Overview
-Epidemiology
Rotator cuff tears (RCTs) are among the most common causes of shoulder pain. Cadaveric and autopsy studies have reported that the prevalence of RCTs ranges from approximately 5% to 40%. Trauma is the predominant etiological factor in younger patients, whereas degenerative processes are more prominent in the elderly population (1).
-Pathophysiology and Biomechanics
Intrinsic and extrinsic mechanisms play a role in the development of chronic degenerative tears. Intrinsic mechanisms are associated with tendon degeneration and hypovascularity. Extrinsic mechanisms include mechanical factors related to subacromial impingement and acromial morphology (2).
Acute rotator cuff tears in the younger population typically occur following a fall. Compared to chronic degenerative tears, tendon quality is better and the potential for repair is higher (3).
The rotator cuff works in conjunction with the deltoid muscle to maintain force balance in the glenohumeral joint and to keep the humeral head centered within the glenoid. In the horizontal plane, there is a balanced force distribution between the subscapularis and the infraspinatus–teres minor complex. The subscapularis plays an important role in anterior flexion, whereas the infraspinatus prevents superior and anterior translation of the humeral head (4).
The rotator cable is a thick bundle of fibers running perpendicular to the supraspinatus tendon and forms the boundary of the rotator crescent, which constitutes the relatively avascular lateral portion of the supraspinatus and infraspinatus tendons. The anterior cable attaches to the greater and lesser tubercles, whereas the posterior cable inserts between the infraspinatus and teres minor. This structure facilitates force transmission and contributes to the preservation of function, particularly in tears involving the crescent region; disruption of the cable may impair shoulder biomechanics and lead to functional loss (5).
- Classification
Rotator cuff tears can be classified according to parameters such as tear depth, size, degree of retraction, and muscle quality. In clinical practice, the most commonly used classifications are based on the distinction between partial- and full-thickness tears, as well as tear size and tendon quality.
Partial-thickness tears involve only a portion of the tendon thickness, whereas full-thickness tears extend through the entire tendon. Partial tears can be subclassified as articular-sided, bursal-sided, and intratendinous, and are most commonly evaluated using the Ellman classification (6).
Full-thickness tears are most commonly classified according to the Cofield classification based on size as small (<1 cm), medium (1–3 cm), large (3–5 cm), and massive (>5 cm) (7). Tendon retraction is evaluated using the Patte classification, while intramuscular fatty degeneration is assessed according to the Goutallier classification.
Additionally, the morphological characteristics of tears (crescent-shaped, U-shaped, and L-shaped) play an important role in surgical planning and in determining the repair technique.
Clinical Presentation
It typically presents with shoulder pain and weakness
Night pain is prominent
Limitation and decreased performance during overhead activities
Pain typically radiates to the lateral aspect of the shoulder and the deltoid region
-Physical Examination
On inspection, muscle atrophy around the shoulder may be observed in chronic cases
On palpation, tenderness may be detected in the subacromial region and over the greater tubercle
Pseudoparalysis: Defined as active elevation of less than 90° with preserved full passive range of motion. It should be evaluated following local anesthetic injection.
Jobe (Empty Can) test | Supraspinatus |
Full Can test | Supraspinatus |
External rotation lag sign | Infraspinatus |
Hornblower sign | Teres minor |
Lift-off test | Subscapularis |
Belly-press test | Subscapularis |
Bear-hug test | Subscapularis |
Imaging
-X-Ray
True AP, AP in internal/external rotation, axillary
Outlet view to assess acromion
· Calcific tendonitis
· Cystic changes in greater tuberosity
· Proximal migration of humerus
· Acromion shape
-MRI
Diagnostic standard for rotator cuff pathology
important to evaluate muscle quality
· Size, shape, and degree of retraction of tear
· Degree of muscle fatty atrophy (best seen on sagittal image)
· Medial biceps tendon subluxation (indicative of a subscapularis tear )
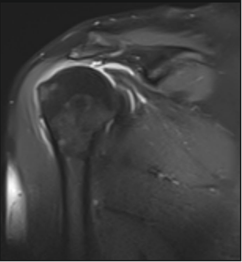
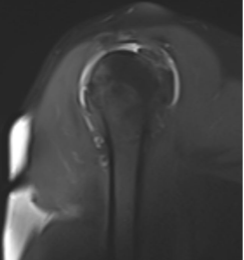
· Tangent sign (failure of the supraspinatus to cross a line drawn between the superior borders of the scapular spine and coracoid process on a sagittal MRI slice)
Massive retracted tear (courtesy of the author)
-Ultrasound
Dynamic examination
Helpful to confirm intraarticular injections
Limited ability to evaluate other intraarticular pathology
Similar sensitivity, specificity, and overall accuracy for diagnosis of rotator cuff disease as compared to MRI
Treatment
Irreparable Rotator Cuff Tears
· Patte stage III tendon retraction
· Goutallier ≥3 fatty degeneration
· Marked muscle atrophy
· Superior migration of the humeral head
· Chronic tear with poor tendon mobility
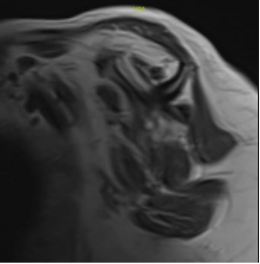
-Fatty degeneration (courtesy of the author)
-Mini-open rotator cuff repair
Once was gold standard but has been largely been replaced by arthroscopic techniques.
-Arthroscopic rotator cuff repair
Single-row and double-row repair- commonly used surgical techniques in rotator cuff repair.
Margin convergence- shown to decrease strain on lateral margin in U shaped tears
Debridement- s procedure involving the removal of degenerative tendon tissue and inflamed subacromial structures aimed at pain relief. In patients with massive or irreparable rotator cuff tears, debridement combined with biceps tenotomy can provide pain relief and symptomatic improvement, particularly in low-demand individuals.
Tuberoplasty- a surgical technique that involves contouring the greater tuberosity to decrease subacromial impingement and provide pain relief, particularly in irreparable rotator cuff tears.
Superior capsular reconstruction- a surgical procedure that utilizes a graft to reconstruct the superior capsule, thereby restoring glenohumeral joint stability and preventing superior humeral head migration in patients with irreparable rotator cuff tears.
Biceps rerouting- a surgical procedure in which the long head of the biceps tendon is rerouted and fixed over the humeral head, functioning as a dynamic restraint to prevent superior migration and improve shoulder stability in irreparable rotator cuff tears.
Biceps superior capsular reconstruction (biceps SCR)- a surgical technique that uses the long head of the biceps tendon as a local autograft to reconstruct the superior capsule, thereby restoring superior stability and preventing humeral head migration in irreparable rotator cuff tears.
-Tendon transfers
Utilized in irreparable rotator cuff tears to restore shoulder biomechanics and function. Latissimus dorsi transfer is traditionally indicated for posterosuperior cuff deficiencies, aiming to improve external rotation and forward elevation, particularly in young and active patients. More recently, lower trapezius transfer has gained popularity due to its more anatomic line of pull, offering improved restoration of external rotation and more favorable shoulder kinematics.
-Reverse shoulder arthroplasty
Indicated in irreparable rotator cuff tears, particularly in the presence of pseudoparalysis or cuff tear arthropathy, aiming to restore shoulder function by medializing the center of rotation and enabling the deltoid to compensate for deficient rotator cuff function.
Prognozis
Prognosis depends on age, tear size, tendon retraction, muscle atrophy, and fatty degeneration.
Smaller tears with minimal retraction are associated with better functional outcomes.
Irreparable rotator cuff tears are associated with poor prognosis.
Marked muscle atrophy and chronic tears are linked to worse outcomes.
Chronic cases are associated with higher re-tear rates.
Differential Diagnosis
· Adhesive capsulitis
· Subacromial impingement syndrome
· Acromioclavicular (AC) joint pathology
· Biceps tendinopathy / SLAP lesions
· Cervical radiculopathy
· Glenohumeral osteoarthritis
· Calcific tendinitis
References
1. Tashjian RZ. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clin Sports Med. 2012;31(4):589-604.
2. Seitz AL, McClure PW, Finucane S, Boardman ND, 3rd, Michener LA. Mechanisms of rotator cuff tendinopathy: intrinsic, extrinsic, or both? Clin Biomech (Bristol). 2011;26(1):1-12.
3. Abdelwahab A, Ahuja N, Iyengar KP, Jain VK, Bakti N, Singh B. Traumatic rotator cuff tears - Current concepts in diagnosis and management. J Clin Orthop Trauma. 2021;18:51-5.
4. Goetti P, Denard PJ, Collin P, Ibrahim M, Hoffmeyer P, Lädermann A. Shoulder biomechanics in normal and selected pathological conditions. EFORT Open Rev. 2020;5(8):508-18.
5. Huri G, Kaymakoglu M, Garbis N. Rotator cable and rotator interval: anatomy, biomechanics and clinical importance. EFORT Open Rev. 2019;4(2):56-62.
6. Ellman H. Diagnosis and treatment of incomplete rotator cuff tears. Clin Orthop Relat Res. 1990(254):64-74.
7. DeOrio JK, Cofield RH. Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am. 1984;66(4):563-7.