Radiologic evaluation of shoulder and elbow disorders is essential for diagnosis, surgical planning, and follow-up. This section outlines the standard imaging modalities and projections used in shoulder and elbow evaluation for musculoskeletal specialists.
I. Imaging Modalities
Conventional Radiography (X-ray)
First-line imaging for both acute and chronic complaints.
Cost-effective and widely available.
Useful for evaluating fractures, dislocations, arthritic changes, and calcific tendinitis.
Computed Tomography (CT)
Superior for osseous anatomy and surgical planning.
3D reconstructions aid in preoperative evaluation, especially for glenoid morphology and complex fractures.
Magnetic Resonance Imaging (MRI)
Preferred for soft tissue pathology, including rotator cuff tears, labral lesions, and marrow edema.
MR arthrography enhances diagnostic accuracy for labral and ligamentous injuries.
Ultrasound
Dynamic assessment of tendons and bursae.
Operator-dependent but valuable for guiding injections and evaluating superficial soft tissue lesions.
II. Shoulder Imaging
Standard Radiographic Views
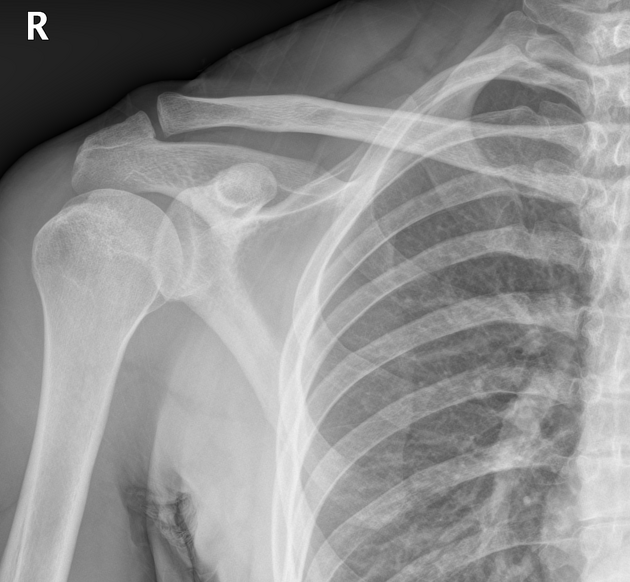
True AP (Grashey View): Visualizes the glenohumeral joint space.
AP Internal/External Rotation: Assesses Hill-Sachs lesions and greater/lesser tuberosity.
Axillary Lateral / Velpeau View: Best for anterior and posterior dislocations.
Scapular Y View: Identifies dislocation direction and scapular fractures.

Specialty Views
Supraspinatus Outlet View (Neer View): Assesses subacromial space and acromion morphology (Bigliani classification).
Zanca View: Enhanced AC joint evaluation.
Stryker Notch View: Detects Hill-Sachs lesions.
West Point View: Anterior glenoid rim and bony Bankart evaluation.
Garth View: Oblique AP projection for glenoid rim and dislocation.
Serendipity View: Sternoclavicular joint visualization.
MRI Protocols
T1-weighted: Anatomy delineation; fat is hyperintense.
T2-weighted with Fat Saturation: Highlights fluid, inflammation, and tears.
STIR: Suppresses fat, highlights edema.
ABER Position (Abduction and External Rotation): Useful in detecting anteroinferior labral injuries and internal impingement.
MR Arthrography: Improves visualization of intra-articular structures, ideal for SLAP, Bankart, and capsular lesions.
CT Utility
Detailed bone assessment (e.g., glenoid version, bone loss).
Preoperative templating for arthroplasty or instability surgery.
III. Elbow Imaging
Standard Radiographic Views
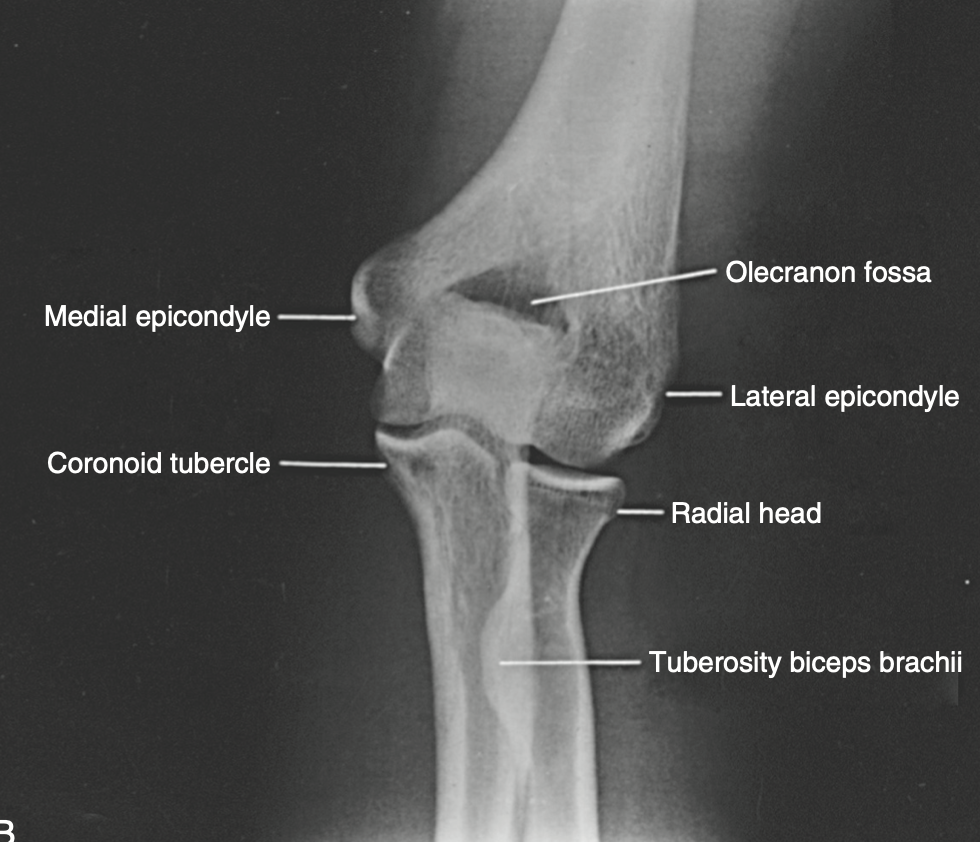
AP View: Assesses joint space, epicondyles, and carrying angle.
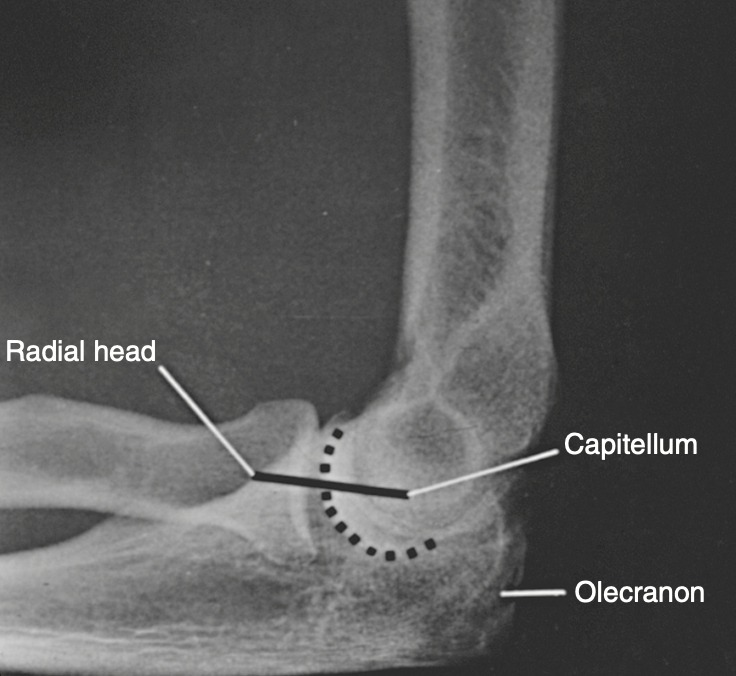
Lateral View: Shows olecranon, anterior/posterior fat pads (effusion sign), and alignment.
Special Views
Oblique Views: Better visualization of radial head and coronoid.
Radial Head-Capitellum View: Focused evaluation for radial head fractures.
Greenspan (Modified Radial Head) View: Visualizes the entire radial head profile.
MRI in Elbow Evaluation
Indicated for evaluating UCL injuries (especially in overhead athletes), osteochondral defects, and soft tissue masses.
T2-weighted fat-sat sequences helpful for edema and ligamentous disruption.
CT and 3D Reconstruction
Used in complex fracture-dislocations, coronoid process fractures, and preoperative planning.
Ultrasound
Evaluation of lateral epicondylitis (common extensor origin), nerve entrapments (e.g., ulnar nerve at cubital tunnel).
IV. Summary
Radiologic imaging of the shoulder and elbow requires a modality-specific and projection-specific approach. Conventional radiographs remain indispensable for primary evaluation, while CT excels in osseous analysis and MRI provides unmatched soft tissue resolution. Understanding the appropriate indications and interpreting key findings across these modalities is essential for guiding diagnosis and treatment in upper extremity pathologies.
References
· Rockwood and matsen's the shoulder, 6th edition
· Morrey's The Elbow and Its Disorders, Fifth Edition