Epidemiology
Accounts for approximately 1–2% of all primary bone tumors.
Most common sites: long bones (femur, tibia, humerus) and posterior elements of the spine.
Less frequently seen in the pelvis, clavicle, or small bones of the hands and feet.
Pathophysiology
The exact etiology remains unclear, but two forms are recognized:
Primary ABC – arises de novo, often associated with a translocation involving the USP6 gene (17p13), leading to osteolytic activity and vascular proliferation.
Secondary ABC – develops in association with another lesion such as giant cell tumor, chondroblastoma, osteoblastoma, or fibrous dysplasia.
The lesion consists of multiple blood-filled spaces without endothelial lining, separated by septa containing fibroblasts, osteoclast-type giant cells, and reactive bone.
Clinical Presentation
Progressive pain, swelling, and restricted motion near the affected site.
Palpable mass may be present.
Pathologic fracture is a common first presentation in long bones.
Neurological deficits can occur when lesions arise in the spine due to canal compression.
Imaging Features
Radiographs:
Expansile, lytic lesion with “blow-out” or balloon-like appearance.
Thin cortical shell and possible septations.
May show fluid–fluid levels if internal hemorrhage is present.
MRI:
Multiple fluid–fluid levels due to different blood degradation stages.
Surrounding bone marrow edema and soft tissue extension are possible.
Contrast enhancement in septa but not in cystic cavities.
CT:
Useful for cortical evaluation and surgical planning.
Histopathology
Multiple cystic spaces filled with blood, lacking endothelial lining.
Septa contain fibroblasts, osteoid tissue, and multinucleated giant cells.
No malignant cells are present.
Differential Diagnosis
Lesion | Type | Distinguishing Features |
|---|---|---|
Telangiectatic Osteosarcoma | Malignant | Malignant cells with nuclear atypia + osteoid production — fluid–fluid levels on MRI with aggressive periosteal reaction |
Giant Cell Tumor (GCT) | Benign aggressive | Occurs after skeletal maturity — epiphyseal, subarticular; lacks fluid–fluid levels; osteoclast-like giant cells throughout |
Chondroblastoma | Benign | Epiphyseal location in skeletally immature — calcifications ("chicken-wire"); chondroblasts + giant cells; perilesional oedema on MRI |
Fibrous Dysplasia | Developmental | Ground-glass matrix on X-ray — no hemorrhagic cavities; shepherd's crook deformity in proximal femur; woven bone in fibrous stroma |
Simple Bone Cyst | Benign | Single unilocular cavity — no septations; metaphyseal / metadiaphyseal; fallen fragment sign on X-ray after pathological fracture |
Aneurysmal Bone Cyst (ABC) | Benign aggressive | Closest mimic — fluid–fluid levels on MRI; septated, expansile; younger patients; no malignant cells or osteoid on histology |
Treatment
Management depends on lesion size, location, and aggressiveness:
Extended curettage and high-speed burring – mainstay for most cases.
Adjuvant therapies to reduce recurrence:Argon beam coagulation, phenol, or liquid nitrogen.
Filling of cavity with bone graft or bone cement.
Selective arterial embolization (SAE) > used for spinal or pelvic lesions or as preoperative adjunct.
Percutaneous sclerotherapy (e.g., doxycycline or polidocanol) is increasingly used as a minimally invasive alternative.
En bloc resection reserved for recurrent or inaccessible lesions.
Prognosis
Recurrence rate: 10–30%, usually within the first two years post-treatment.
Risk factors for recurrence include younger age, open physes, and incomplete excision.
Long-term prognosis is excellent with appropriate treatment; malignant transformation is exceedingly rare.
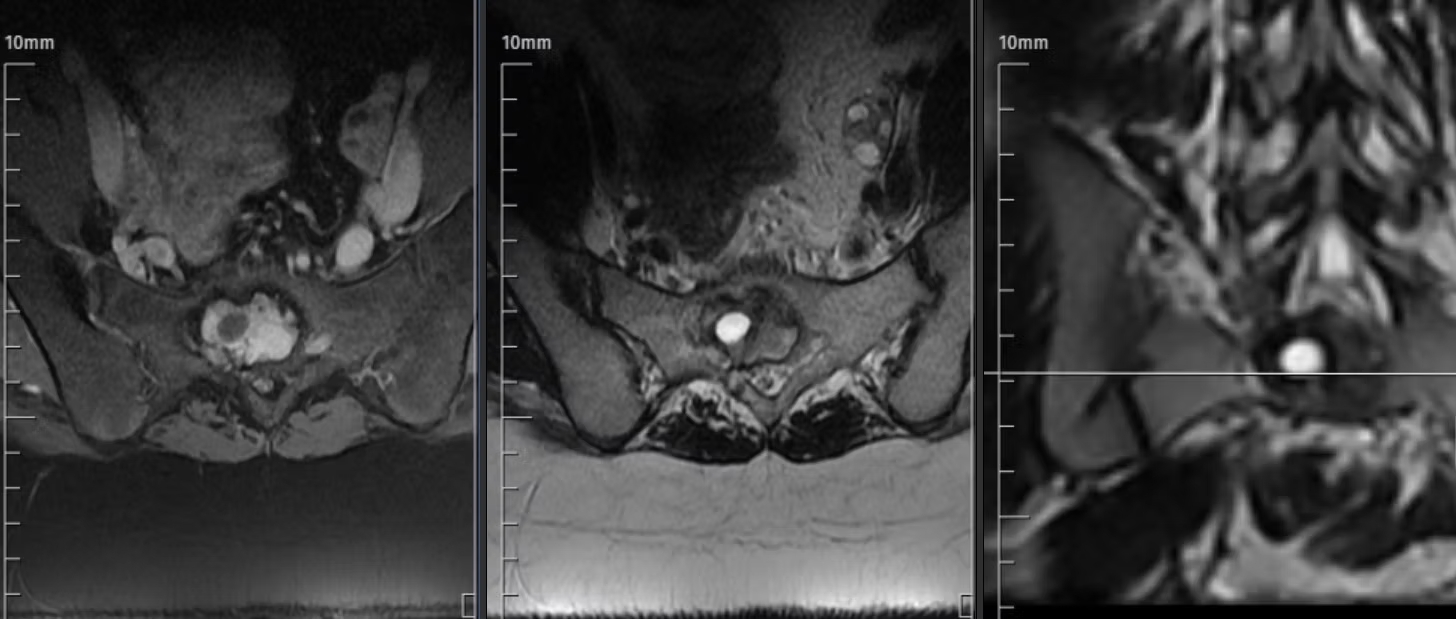
Axial and coronal MRI images of the sacrum demonstrate an expansile, multiloculated cystic lesion centered at the S1 level. The lesion shows multiple fluid–fluid levels with low-to-intermediate signal on T1-weighted, high signal on T2-weighted images, and thin peripheral and septal enhancement after gadolinium administration. Imaging features are characteristic of a benign aneurysmal bone cyst without evidence of solid enhancement or soft-tissue invasion.
Key Points
ABC is a benign, vascular, expansile bone lesion with locally destructive potential.
USP6 translocation confirms diagnosis in ambiguous cases.
Fluid–fluid levels on MRI are suggestive but not pathognomonic.
Minimally invasive approaches (e.g., sclerotherapy, embolization) show recurrence rates comparable to surgery in recent studies.
Extended curettage with adjuvant remains the gold standard for accessible lesions in long bones.
Recurrent cases may benefit from a combined strategy (embolization > curettage > bone graft).
References
Oliveira AM et al. USP6 Gene Rearrangement in Aneurysmal Bone Cyst. Am J Pathol. 2021;191(7):1210–1220.
Mascard E, Gomez-Brouchet A, Lambot K. Aneurysmal Bone Cyst: Clinical and Therapeutic Update. Orthop Traumatol Surg Res. 2015;101(1 Suppl)–S19.
Park HY et al. Treatment of Aneurysmal Bone Cysts: A Review of Current Concepts. J Bone Joint Surg Am. 2020;102(4):280–289.
Rastogi S et al. Percutaneous Doxycycline Sclerotherapy in Aneurysmal Bone Cyst. J Orthop Surg. 2019;27(3):2309499019878422.
Rapp TB et al. Aneurysmal Bone Cyst: A Review of Pathophysiology and Current Management. J Am Acad Orthop Surg. 2012;20(4):233–241