Definition
Management of segmental bone defects resulting from:
Trauma
Infection
Tumour resection
Requires restoration of:
Mechanical stability
Biological environment
Key Principle
Stability + vascularity + infection control = success
Treatment Determinants
Defect size
Infection status
Soft tissue condition
Patient compliance
Main Techniques
1. Masquelet Technique (Induced Membrane)
Concept
Two-stage reconstruction using a biologically active induced membrane
Stage 1
Radical debridement
PMMA spacer placement (± antibiotics)
Stabilisation
Membrane forms around spacer
Stage 2 (4–8 weeks)
Remove spacer
Preserve membrane
Fill defect with bone graft
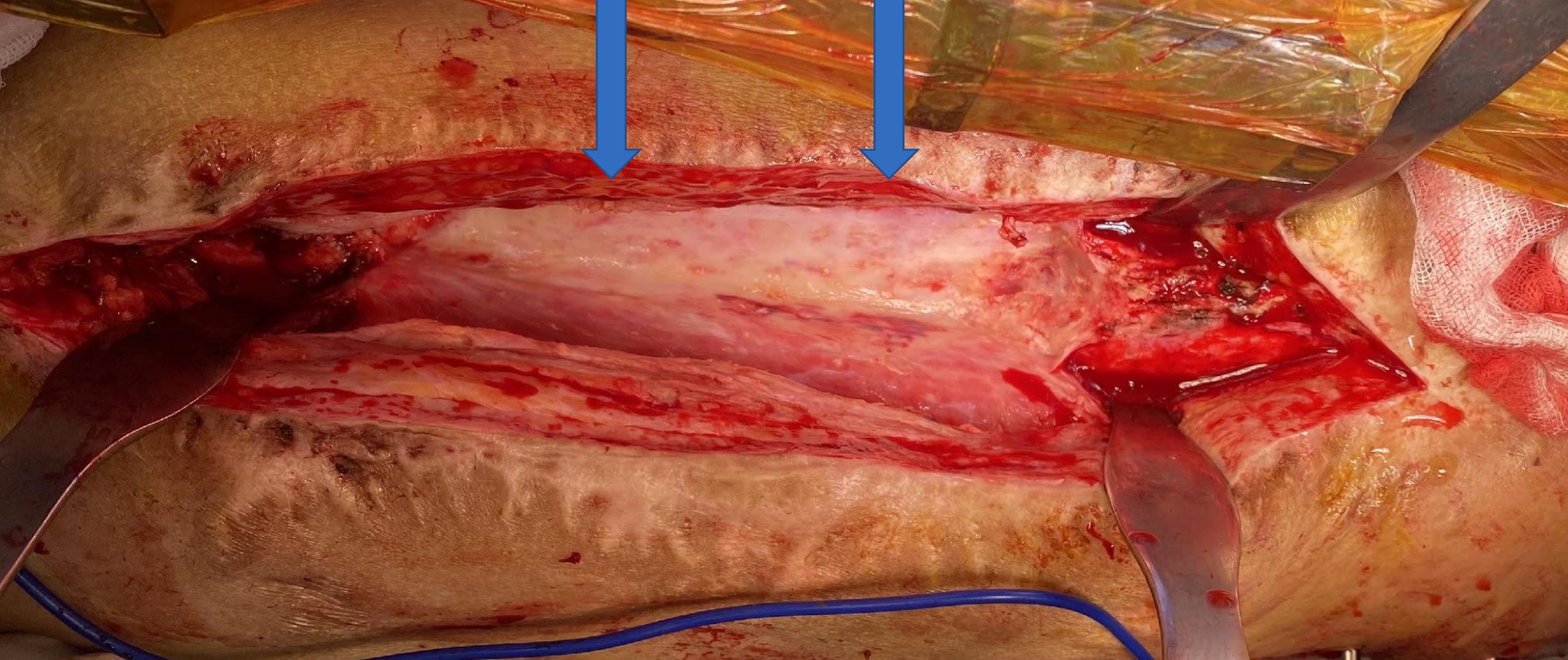
Biological Insight (Key Advantage)
Induced membrane is:
Hypervascular (~32.8 vessels/mm²)
Thick (~2.4 mm)
Rich in collagen type I
Acts as a biological chamber, not true periosteum
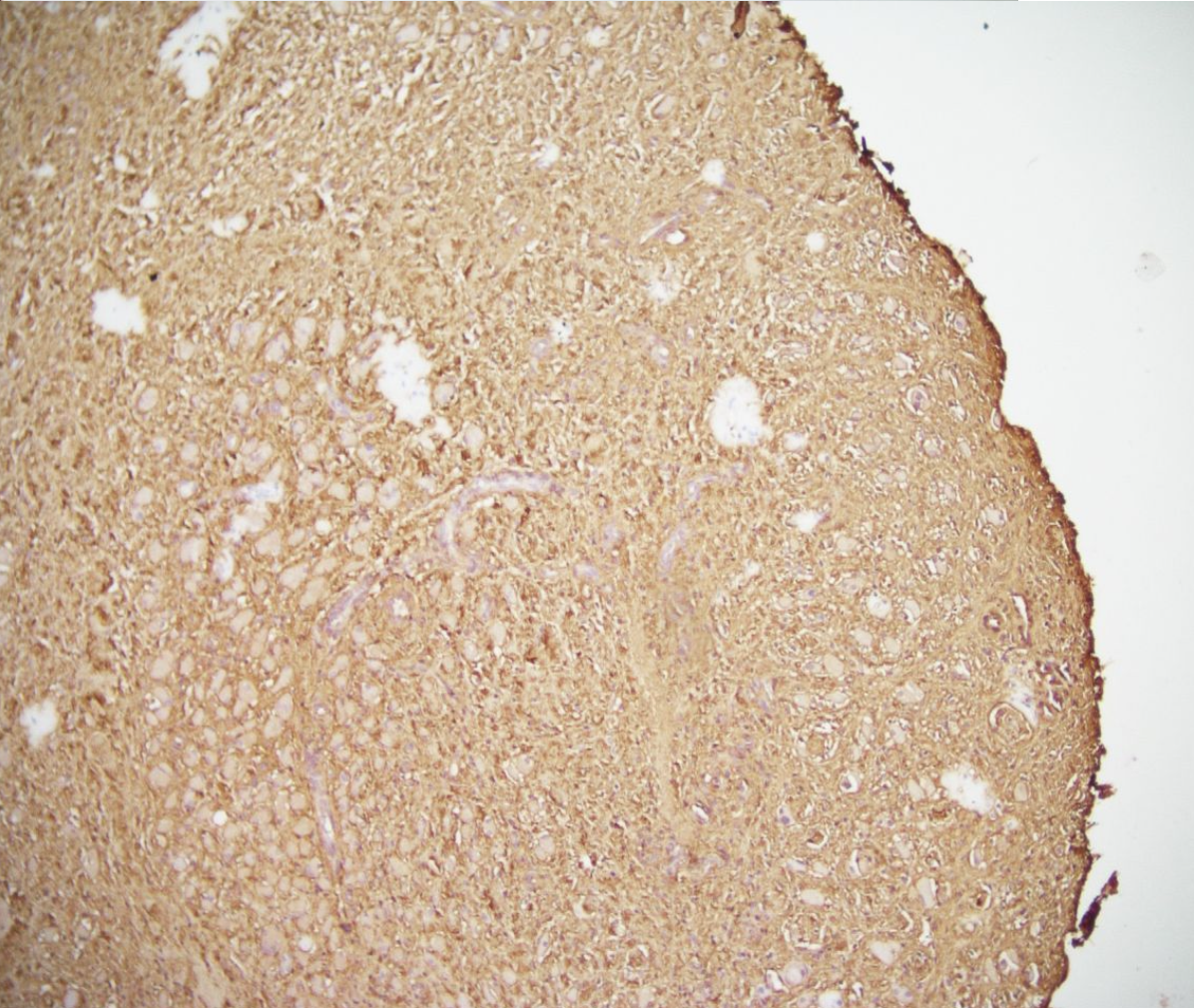
Collagen Type I
Advantages
Technically simpler
Shorter learning curve
Effective in infected cases
Good for moderate defects (2–5 cm)
Limitations
Requires sufficient bone graft
Two-stage procedure
Less effective in very large defects
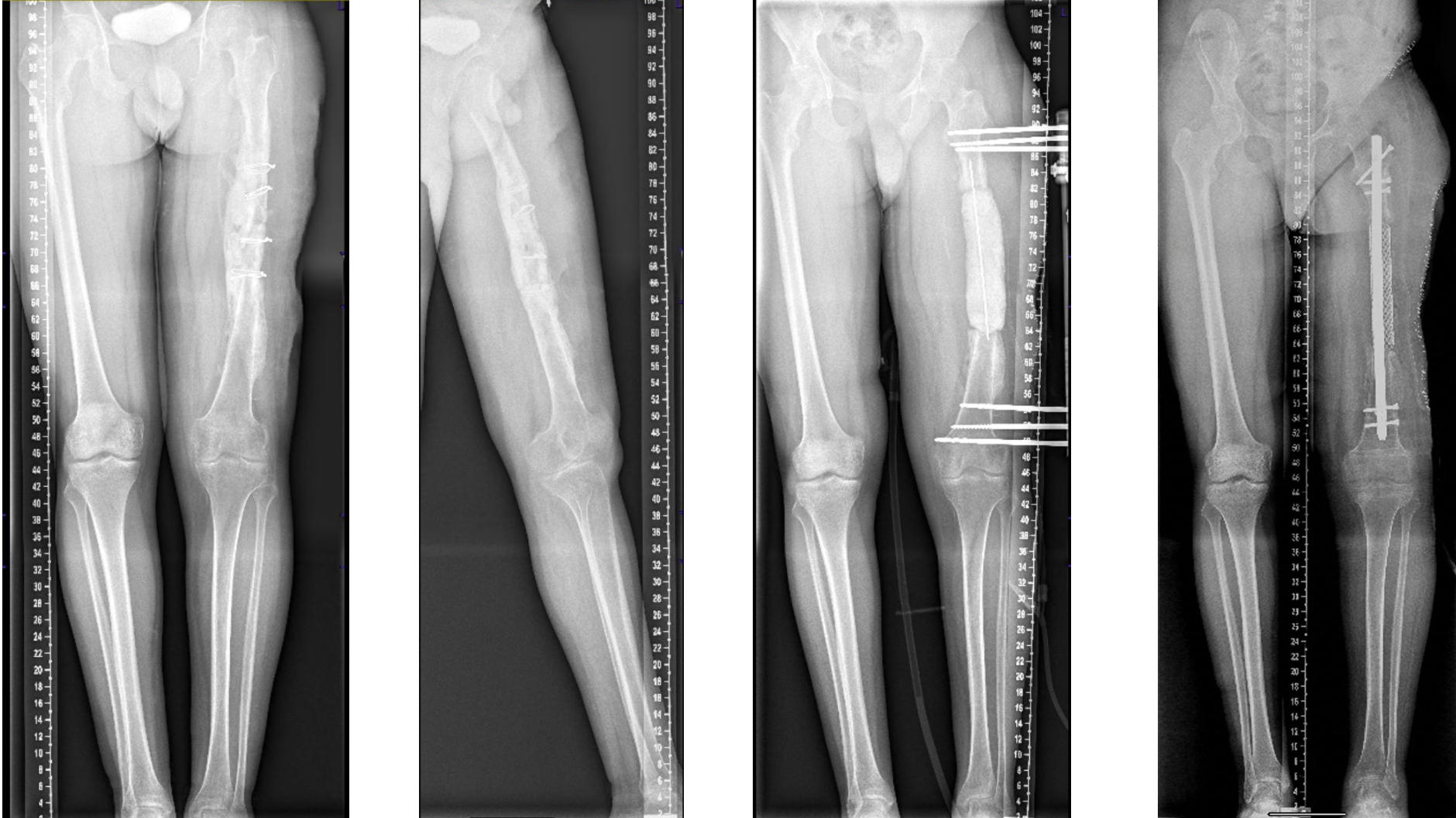
2. Bone Transport (Ilizarov Method)
Concept
Gradual bone regeneration via distraction osteogenesis
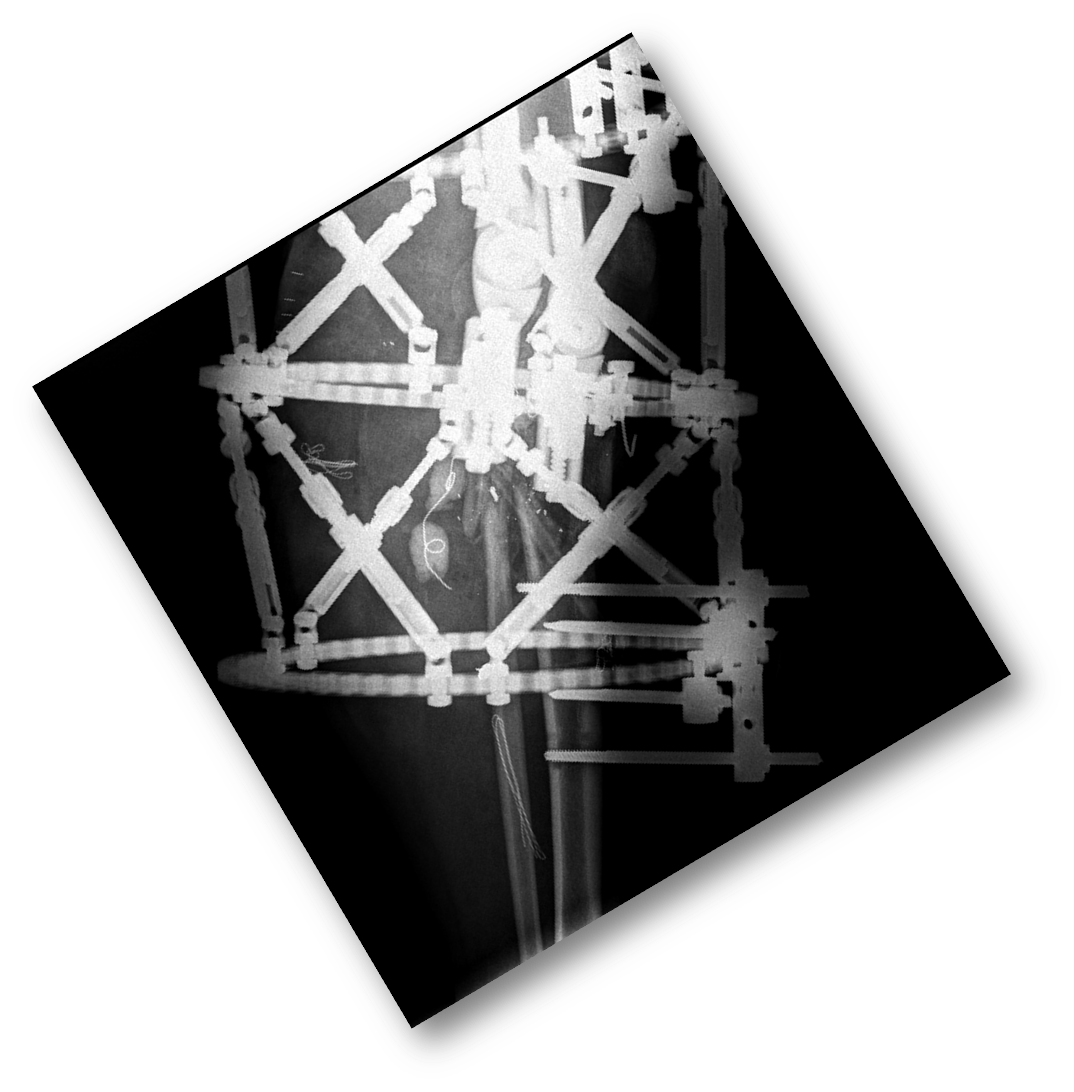
Technique
Osteotomy performed
Bone segment transported across defect
New bone forms in distraction gap
Advantages
Ideal for large defects (>5 cm)
No need for large graft
Can correct deformity simultaneously
Limitations
Long treatment duration
High patient burden
Requires strong compliance
Pin site complications common
Complications (Both Techniques)
Infection
Joint stiffness
Malalignment
Psychological burden
Comparison Table
Feature | Masquelet | Bone Transport (Ilizarov) |
|---|---|---|
Stages | Two-stage | Continuous process |
Ideal defect size | 2–5 cm | >5 cm |
Graft requirement | Yes | No |
Duration | Shorter | Longer |
Technical difficulty | Moderate | High |
Patient burden | Lower | Higher |
Infection control | Good | Good |
Masquelet = biological optimisation strategy
Ilizarov = mechanical regeneration strategy
The real difference:
Masquelet depends on graft biology
Transport depends on host regenerative capacity
Pits & Pearls
Soft tissue status determines success more than technique
Infection control is always first step
Masquelet membrane must be preserved
Ilizarov requires patient commitment
Pitfalls
Choosing technique based only on defect size
Ignoring soft tissue envelope
Poor fixation strategy
Underestimating patient compliance
Comparison: Masquelet vs Bone Transport
Feature | Masquelet | Bone Transport (Ilizarov) |
|---|---|---|
Stages | Two-stage | Single continuous process |
Ideal defect size | 2–5 cm | >5 cm |
Graft requirement | Yes | No |
Duration | Shorter | Longer |
Technical difficulty | Moderate | High |
Patient burden | Lower | Higher |
Infection control | Good | Good |
Mini Decision Algorithm
Condition | Decision | Action |
|---|---|---|
Defect ≤ 5 cm | Technique | Masquelet |
Defect > 5 cm | Technique | Bone transport |
Infection present | First | Debridement first |
Poor compliance | Avoid | Ilizarov |
Soft tissue problem | Priority | Address before reconstruction |