Spinal Neurological Assessment (Spot Knowledge)
General Principles
Includes motor, sensory, and reflex exam of all extremities
Use Manual Muscle Testing (0–5 scale) for consistency
Reflexes graded as: 0 = absent, 1+ = diminished, 2+ = normal, 3+ = brisk, 4+ = clonus
Upper Extremity
Motor
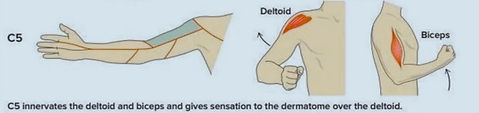
C5 – Shoulder abduction (deltoid), elbow flexion (biceps)
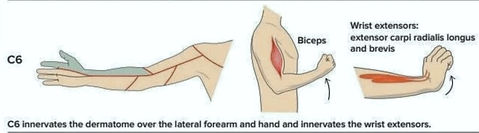
C6 – Elbow flexion, wrist extension
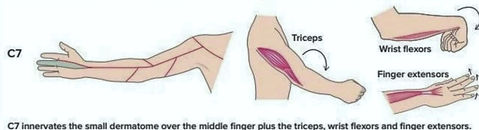
C7 – Elbow extension (triceps), wrist flexion
C8 – Finger flexion
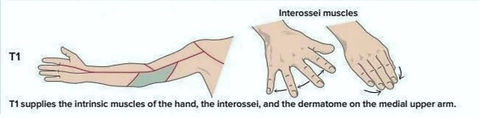
T1 – Finger abduction (intrinsic muscles)
💡 Grip (C8) and finger abduction (T1) often early affected in cervical radiculopathy
Sensory
C5 – Lateral shoulder
C6 – Radial forearm, thumb
C7 – Middle finger
C8 – Little finger, ulnar hand
T1 – Medial forearm
Reflexes
C5–C6: Biceps → elbow flexion
C6: Brachioradialis → elbow flexion, forearm supination
C7: Triceps → elbow extension
Special Tests
Spurling: axial load with neck extension/lat. flexion → radicular pain = positive
Lhermitte: electric-shock sensation with neck flexion → cervical myelopathy
Hoffman: flicking distal phalanx of middle finger → thumb flexion/adduction = UMN sign
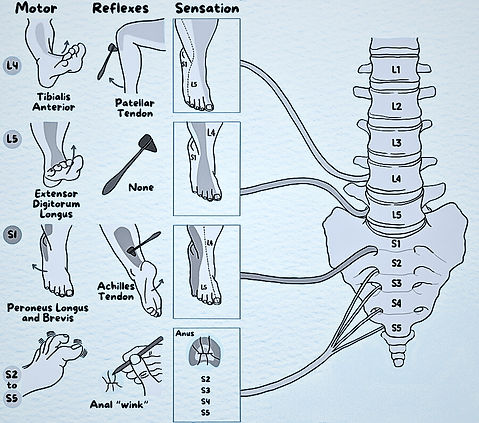
Lower Extremity
Motor
L2 – Hip flexion
L3 – Knee extension
L4 – Ankle dorsiflexion
L5 – Great toe extension (EHL)
S1 – Plantar flexion, eversion
S2 – Knee flexion
💡 L5 weakness → cannot heel walk; S1 weakness → cannot toe walk
Sensory
L2 – Anterior thigh
L3 – Knee region
L4 – Medial leg/ankle
L5 – Dorsum of foot, great toe
S1 – Lateral foot, little toe
S2 – Posterior thigh
Reflexes
L4: Patellar (quadriceps)
S1: Achilles (gastrosoleus)
Pathological:
Babinski – great toe dorsiflexion = UMN sign
Clonus – rhythmic ankle beats with forced dorsiflexion = UMN sign
Chaddock/Oppenheim – Babinski equivalents
Special Tests
SLR (Lasègue): 30–70° → radicular pain = L4–S1 compression
Bragard: pain reappears with ankle dorsiflexion after SLR
Cross Lasègue: contralateral leg raising provokes pain → severe root compression
Femoral Nerve Stretch: prone, knee flexion → anterior thigh pain = L2–L4 compression
Clinical Pearls
Always check sacral segments (S4–S5) → anal tone, perianal sensation, bulbocavernosus reflex
Document systematically (ASIA/ISCoS standards if possible)
Radiculopathy → loss of reflex in affected root
Myelopathy → hyperreflexia + pathological reflexes
References
American Spinal Injury Association (ASIA). International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI). 2022.
Hoppenfeld S, DeBoer P. Examination of the Spine and Extremities. Appleton & Lange, 1976.
Fehlings MG, Tetreault LA, et al. Assessment of spinal cord injury and myelopathy. Lancet Neurol. 2017;16(6):482–492.
Dumitru D, Amato AA, Zwarts MJ. Electrodiagnostic Medicine. 2nd ed. Hanley & Belfus, 2002.
Kendall FP, et al. Muscles: Testing and Function with Posture and Pain. 6th ed. Lippincott Williams & Wilkins, 2020.