Overview
● Traumatic injuries to the occipitocervical junction (OCJ) span a spectrum from isolated, nondisplaced occipital condyle fractures to complete occipitocervical dislocations.
● The increased use of advanced imaging, specifically Computed Tomography (CT) and Magnetic Resonance Imaging (MRI), has led to improved recognition, classification, and contemporary treatment protocols.
● Optimal management is contingent upon a thorough understanding of the unique regional anatomy, precise radiographic criteria, and reliable surgical stabilization techniques.
Anatomy and Biomechanics
● The OCJ, composed of the cranial occipital bone, atlas (C1), and axis (C2), forms an integrated functional unit.
● Kinematics :
○ The occipitocervical junction is highly mobile, accounting for approximately 60% of axial-plane cervical spine rotation and 40% of sagittal-plane
flexion-extension motion.
○ Overall, this region is responsible for 45% of the total neck motion.
● Structural Stability:
○ The extensive range of motion is facilitated by a joint architecture that inherently possesses relatively few bony constraints.
○ Consequently, strong ligamentous support is critical to prevent excessive motion and structural failure in this region.
○ The integrity of these ligaments is paramount due to the proximity of vulnerable neurovascular structures.
● Primary Ligamentous Stabilizers:
○ The cruciate ligament, alar ligaments, and tectorial membrane collectively function as the primary ligamentous stabilizers of the occipitoatlantal joint.
● Tectorial Membrane: This is an upward extension of the posterior longitudinal ligament. It acts as a major stabilizer for the OCJ, primarily by limiting axial distraction and atlanto-occipital flexion.
● Alar Ligaments: Originating from the superior posterior surface of the dens, they insert onto the medial border of the occipital condyles and the lateral masses of C1. They are considered crucial as the main restraint to axial rotation in the upper cervical spine.
● Cruciate Ligament: This structure forms a cross-like arrangement behind the dens. Its transverse portion plays a significant role in axial rotation and lateral bending of the C1-C2 joints and also restrains head flexion during motion.
Imaging
● Plain radiographic evaluation of the cervical spine is generally insufficient for consistent and adequate diagnosis of occipital condyle fractures and has disadvantages when assessing the upper cervical spine.
● All patients suspected of having an occipital condyle injury should be evaluated with Computed Tomography (CT).
● Magnetic Resonance Imaging (MRI) of the craniovertebral junction is classically indicated for patients with spinal cord injury to assess upper cervical spine ligamentous injuries and hemorrhage.
● Diagnostic Criteria (Adults):
○ Basion-Dens Interval (BDI): The distance from the basion to the upper tip of the odontoid is considered abnormal if it measures >12mm (Harris method).
○ Basion-Axial Interval (BAI): The basion is considered to lie abnormally if it is >4 mm anterior or >12 mm posterior to a line projecting cranially from the posterior cortex of the C2 vertebral body.
○ The BDI and BAI, when used together (Harris lines), have significantly higher sensitivity and specificity compared to the Powers' ratio.
○ Condylar Gap Method (Occipital Condyle-C1 Interval): The distance between the occipital condyle and the superior articular facet of the atlas is considered abnormal if it is >2 mm in adults.
○ Powers' Ratio:
■ This ratio is considered abnormal if the ratio of the distance from the basion to the posterior cortex of the atlas (AB) and the distance from the opisthion to the anterior arch of the atlas (CD) is >1.
■ Its use is limited only to cases of anterior occipitocervical dislocation.
■ The Powers' ratio has low sensitivity and specificity compared to the BDI and BAI methods.
Classification
1. Occipital Condyle Fractures (Anderson & Montesano):
● Type I (Impaction): Comminuted fracture due to axial loading. Usually stable
● Type II (Basilar): Extension of a linear skull base fracture into the condyle (shear mechanism). Usually stable
● Type III (Avulsion): Avulsion fracture at the alar ligament attachment due to rotation/lateral bending. Potentially unstable
2. Occipitocervical Dislocation (Traynelis):
● Type I: Anterior displacement of occiput relative to atlas.
● Type II: Longitudinal distraction (vertical).
● Type III: Posterior displacement.
3. Harborview Classification (MRI-Based)
This system is particularly useful for determining stability in non-displaced or subtly displaced injuries.
● Stage 1: MRI signal abnormality with <2 mm of distraction. Typically managed nonoperatively with a rigid collar or halo vest.
● Stage 2: >2 mm distraction demonstrated on traction. Considered unstable and requires surgical fixation.
● Stage 3: Static displacement >2 mm. Represents overt instability and mandates surgical stabilization.
Treatment
● Conservative Management:
○ Indication: Stable injuries, including Anderson & Montesano Type I and Type II fractures.
○ Contraindication: Cervical traction is contraindicated in suspected Type C (dissociative) injuries, as it may exacerbate distraction and result in catastrophic neurological injury, including spinal cord transection.
○ Protocol: Rigid cervical collar is typically sufficient. Halos are rarely used for stable fractures.
● Surgical Management:
○ Indication: Occipitocervical instability (Type III condyle fractures, dislocations) and presence of neurological deficits.
○ Technique: Posterior Occipitocervical Fusion is the standard.
○ Screw-Rod Constructs: Preferred over wiring/cables due to superior biomechanical stability and reduced need for postoperative halo immobilization.
○ Fixation Points: Typically involves an occipital plate and screws in C1 (lateral mass) and C2 (pedicle/pars/translaminar).
○ Outcomes: Fusion rates are high (89-100%). Pain reduction is achieved in 78-95% of patients
Differential Diagnosis
● Atlantoaxial rotatory subluxation (AARS)
● Odontoid fractures (Type II and III)
● C1 burst fracture (Jefferson fracture)
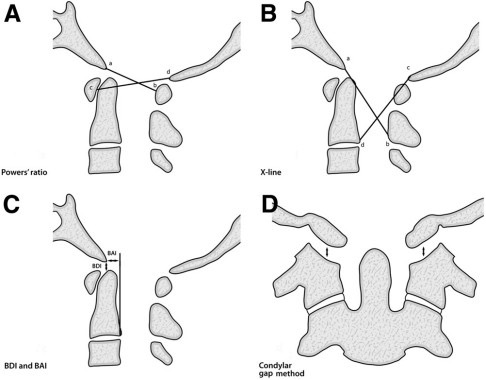
Radiologic diagnostic methods for occipitocervical dislocations: (A) Powers' ratio, (B) X-line method, (C) Basion-Dens Interval (BDI) and Basion-Axial Interval (BAI) (Harris lines), and (D) Condylar gap method.
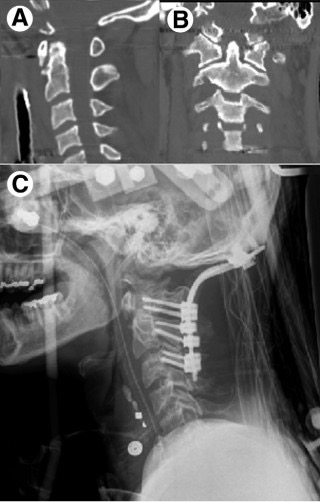
Case of a 27-year-old man with occipitocervical injury: (A) Sagittal view showing clivus fracture, (B) Coronal view showing bilateral occipital condyle fracture, and (C) Post-operative occiput-C3 fusion.
References
1. Smorgick Y, Fischgrund JS. "Occipitocervical Injuries." Seminars in Spine Surgery, 2013;25:14-22.
2. Anderson PA, Montesano PX. "Morphology and treatment of occipital condyle fractures." Spine, 1988;13:731-736.
3. Kasliwal MK, Fontes RB, Traynelis VC. Occipitocervical dissociation-incidence, evaluation, and treatment. Curr Rev Musculoskelet Med. 2016 Sep;9(3):247-54. doi: 10.1007/s12178-016-9347-6. PMID: 27255101; PMCID: PMC4958379.
4. Harris JH Jr, et al. "Radiologic diagnosis of traumatic occipitovertebral dissociation." AJR Am J Roentgenol, 1994;162:887-892.
5. Dvorak J, et al. "Biomechanics of the craniocervical region: The alar and the transverse ligaments." Journal of Orthopaedic Research, 1988;6:452-461.