Epidemiology
Bimodal age distribution:
Adolescents (10–20y): Most common (~75%)
Elderly (>65y): Often secondary to Paget’s, radiation, infarctM:F = 1.5:1
Peak incidence: Distal femur > Proximal tibia > Proximal humerusEpidemiology
Bimodal age distribution:
Adolescents (10–20y): Most common (~75%)
Elderly (>65y): Often secondary to Paget’s, radiation, infarctM:F = 1.5:1
Peak incidence: Distal femur > Proximal tibia > Proximal humerus
Aetiology & Genetics
Mostly sporadic
Associated tumor suppressor mutations:
RB gene (Retinoblastoma)
TP53 (Li-Fraumeni syndrome)Rare hereditary syndromes:
Rothmund-Thomson, Bloom, Werner
Histology
Malignant mesenchymal spindle cells producing lace-like osteoid
High N:C ratio, nuclear atypia, mitoses
Diagnostic criteria:
Malignant stroma
Osteoid production
Subtypes
INTRAMEDULLARY
Conventional (high-grade)
Telangiectatic
Small-cell
Low-grade variants
SURFACE
Parosteal (low-grade)
Periosteal (intermediate-grade)
Dedifferentiated surface (high-grade)
OTHERS
Intracortical (rarest)
Extraskeletal (soft tissue OSA, rare, radiosensitive)
Clinical Features
Progressive pain + swelling, often attributed to trauma
Night/rest pain common
Mass effect, ↓ROM, neurovascular compromise possible
Median delay to diagnosis: ~4 months
Imaging
X-ray:
Mixed lytic–blastic lesion
Sunburst, Codman’s triangle, “Hair-on-end”
Cortical destruction + soft tissue extension
MRI:
Assess extent, skip lesions, neurovascular invasion
Includes entire bone
CT Chest:
Mandatory for lung metastasis detection
Bone scan / PET-CT:
Staging, skip lesions
Staging
Most are Enneking Stage IIB (high grade, extracompartmental, no mets)
Stage III if lung/bone mets
Skip lesions → considered metastasis
Differential Diagnosis
Ewing sarcoma (t(11;22), small round blue cells)
Osteomyelitis (sequestrum, Brodie abscess)
ABC (vs Telangiectatic OSA)
Fibrosarcoma, Lymphoma, EG, Leukemia
Labs
↑ ALP & LDH → indicator of high tumor burden
Histological response post-chemo:
>90% necrosis = good prognosis
Biopsy
Core biopsy by definitive surgeon
Incorrect biopsy track → ↑amputation risk
Treatment
1. Neoadjuvant chemotherapy
8–12 weeks: MAP regimen (Methotrexate + Doxorubicin + Cisplatin ± Ifosfamide)
2. Wide resection
Limb-salvage preferred
Criteria: good chemo response, resectable margins
3. Reconstruction options
Endoprosthesis
Allograft/autograft
Rotationplasty (esp. in children with extensive disease)
Amputation (if salvage not possible)
4. Adjuvant chemotherapy
Continue for 6–12 months post-op
Radiation
OSA = radioresistant
Reserved for:
Extraskeletal OSA
Palliative settings
Spine/pelvis with close margins
Complications
Limb salvage:
Prosthetic infection (2–10%)
Aseptic loosening (esp. tibia)
Nonunion/fracture of grafts
Local recurrence
Rotationplasty:
Malrotation
Vascular compromise
Cosmesis concerns
Amputation:
Neuroma, phantom pain, wound healing
Prognosis
5-yr survival (localized):
~85% (good chemo response)
~65% (general)5-yr survival (metastatic):
~20% with pulmonary mets
Bone mets = poor outcomePrognostic factors:
Response to chemo
Stage at diagnosis
ALP/LDH levels
Tumor size/location
Surgical margins
VEGF or MDR expression
Clinical Features
Progressive pain + swelling, often attributed to trauma
Night/rest pain common
Mass effect, ↓ROM, neurovascular compromise possible
Median delay to diagnosis: ~4 months
References:
Whelan JS, Davis LE. Osteosarcoma: Biology, diagnosis, and treatment strategies.Current Oncology Reports. 2018;20(1):2.
[DOI: 10.1007/s11912-018-0652-0]Isakoff MS, Bielack SS, Meltzer P, Gorlick R.Osteosarcoma: Current treatment and a collaborative pathway to success. J Clin Oncol. 2015;33(27):3029–3035.[DOI: 10.1200/JCO.2014.59.4895]
Orthopaedic Knowledge Update: Musculoskeletal Tumors 4. Eds: Letson GD, Mankin HJ.American Academy of Orthopaedic Surgeons (AAOS), 2016.
WHO Classification of Tumours Editorial Board.Soft Tissue and Bone Tumours. WHO Classification of Tumours, 5th Edition, Volume 3.
International Agency for Research on Cancer (IARC); 2020.Peabody TD, Attar S, eds.Orthopaedic Oncology: Primary and Metastatic Tumors of the Skeletal System.Cancer Treatment and Research Series. Springer; [Indexed in PubMed/Medline].
Category | Subtype | Features |
Intramedullary | Conventional Osteosarcoma | Heterogeneous histology: may contain cartilaginous, fibrous, giant cell, or small round blue cell components. |
Telangiectatic Osteosarcoma | Resembles aneurysmal bone cyst; blood-filled cavities with scant osteoid lining. | |
Small-cell | Overlaps with Ewing sarcoma; small round blue cells producing immature osteoid. | |
Fibrous dysplasia-like | High-volume fibrous stroma + immature osteoid. | |
Desmoplastic fibroma-like | Low-volume fibrous stroma + immature osteoid. | |
Surface | Parosteal Osteosarcoma | Low-grade; arises from outer periosteal layer. |
Periosteal Osteosarcoma | Intermediate-grade; from between bone surface and inner periosteum. | |
Dedifferentiated surface | High-grade surface variant. | |
Intracortical | Intracortical Osteosarcoma | Extremely rare; arises within cortical bone. |
Extraskeletal | Extraskeletal Osteosarcoma | Soft tissue origin; <5% of all cases; requires wide resection and radiation. |

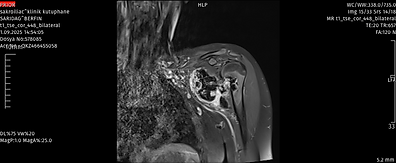
Xray and Mri of the proximal humerus bone tumor
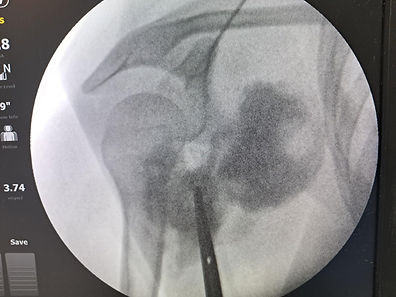
Biopsy fluoroscopy image

Surgery plan drawings
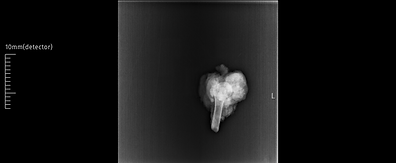
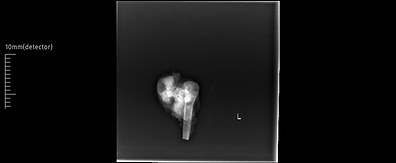
Xray of the resected humerus

Pathologic specimen
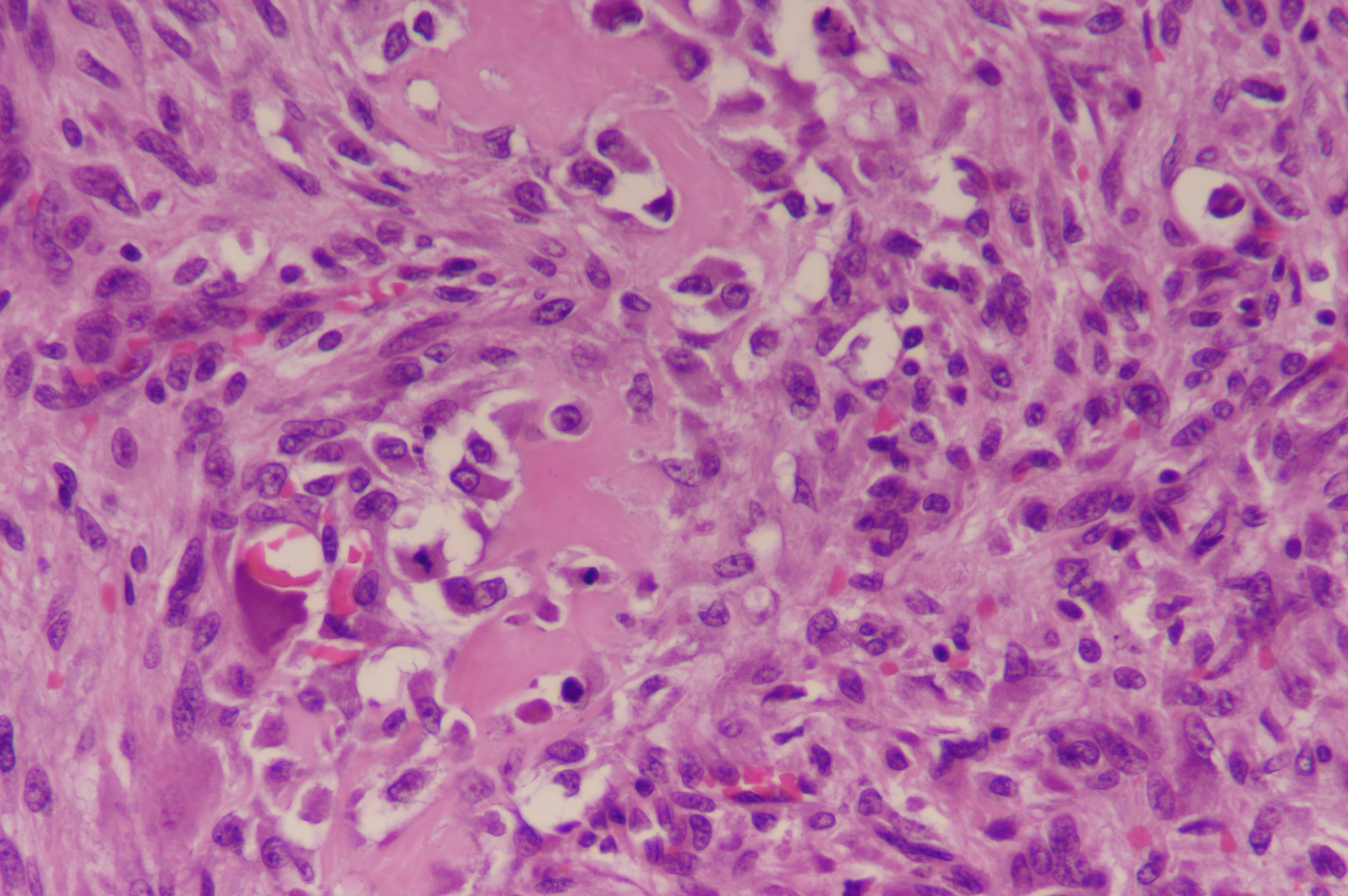
Osteosarcoma pathology

Postoperative total shoulder tumor prosthesis