Epidemiology
Incidence: approximately 1.8 cases per million per year.
Most common in adults aged 30–50 years.
Slight female predominance.
Knee is affected in about 75% of cases, followed by hip, ankle, and shoulder.
Pathophysiology
Thought to arise from clonal neoplastic proliferation of synovial cells driven by CSF1 gene overexpression due to a t(1;2)(p13;q37) translocation.
Overproduction of colony-stimulating factor 1 (CSF1) recruits macrophages and giant cells, leading to synovial hyperplasia and hemosiderin deposition.
Classified into two forms:Localized (Nodular) PVNS – affects tendon sheaths, often in the hand or foot.
Diffuse PVNS – involves entire synovial lining of large joints, most commonly the knee or hip.
Clinical Presentation
Gradual joint swelling, pain, and stiffness over months or years.
Recurrent hemarthrosis (bloody effusion) is a classic finding.
Mechanical symptoms (locking or catching) in large joints due to nodular tissue.
In advanced disease, cartilage erosion and secondary osteoarthritis may occur.
Imaging Features
Radiographs:
Often normal in early stages.
Later show periarticular bone erosions with preserved joint space.
MRI (gold standard):
Diffuse synovial thickening with low signal intensity on both T1 and T2 (due to hemosiderin).
“Blooming artifact” on gradient-echo sequences is characteristic.
Contrast enhancement demonstrates active synovial proliferation.
CT Scan:
Useful to assess bone erosion and subchondral involvement.
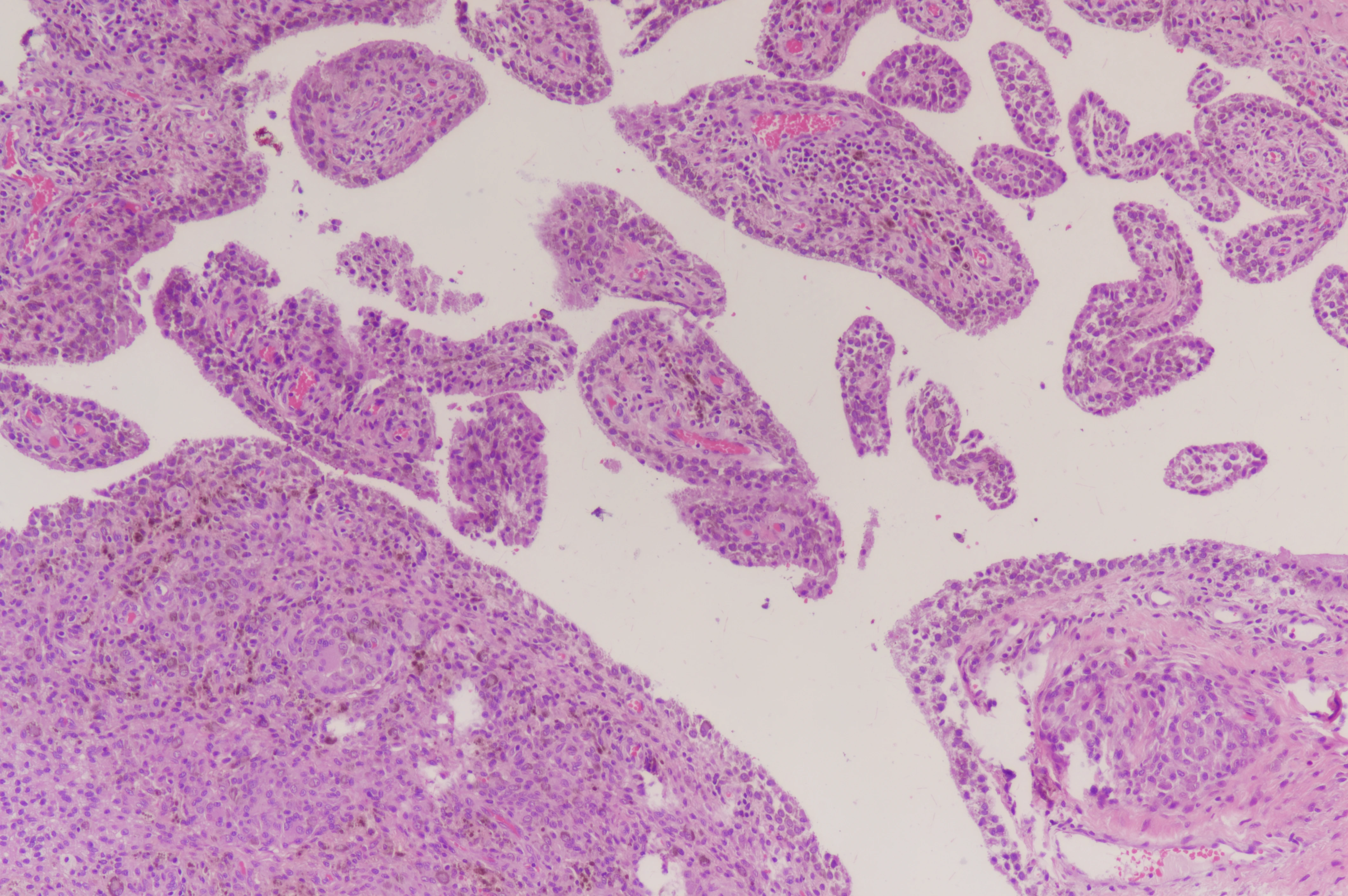
Histopathology
Synovial villi and nodules composed of mononuclear histiocyte-like cells, multinucleated giant cells, foam cells, and hemosiderin deposits.
Mitotic activity is present but without atypia or malignant features.
Differential Diagnosis
Condition Distinguishing Feature
Rheumatoid arthritis : Bilateral, symmetric, elevated serologic markers
Hemophilic arthropathy : History of bleeding disorder, absence of proliferative nodules
Synovial chondromatosis : Cartilaginous nodules visible on imaging
Synovial sarcoma : Malignant histology, soft-tissue mass, calcifications
Treatment
The mainstay of treatment is complete synovectomy, with the goal of eradicating diseased synovium while preserving joint function.
1. Surgical Management
Arthroscopic synovectomy – preferred for localized or accessible diffuse disease.
Open synovectomy – required for extensive or extra-articular extension.
Combined approach (open + arthroscopic) may reduce recurrence in the knee.
Joint replacement (arthroplasty) indicated in end-stage degenerative joints.
2. Adjuvant Therapies
External beam radiotherapy (EBRT) or radiosynovectomy (Yttrium-90) can reduce recurrence after incomplete resection.
Targeted therapy: CSF1 receptor inhibitors (e.g., Pexidartinib) are effective for unresectable or recurrent cases.
Prognosis
Localized PVNS: recurrence <10%.
Diffuse PVNS: recurrence 20–50%, often within 2 years.
Delayed diagnosis or incomplete excision can lead to joint destruction requiring arthroplasty.
Metastasis is exceptionally rare.
Key Points
PVNS is a benign but destructive synovial tumor driven by CSF1 overexpression.
MRI blooming artifact is a key diagnostic feature.
Complete synovectomy remains the gold standard treatment.
Targeted CSF1 inhibitors offer new hope for recurrent or unresectable cases.
Localized PVNS → Arthroscopic excision gives excellent outcomes with minimal recurrence.
Diffuse PVNS → Combined synovectomy ± adjuvant therapy provides better local control.
CSF1R inhibitors (e.g., Pexidartinib) are now first-line for unresectable or recurrent diffuse PVNS.
References
Mastboom MJL, et al. Diffuse-Type Tenosynovial Giant Cell Tumor: Current Concepts and Future Perspectives. Nat Rev Rheumatol. 2021;17(6):363–376.
Cassier PA, et al. CSF1R Inhibition with Pexidartinib in Tenosynovial Giant Cell Tumor. N Engl J Med. 2019;379(4):341–350.
van der Heijden L, et al. Pigmented Villonodular Synovitis: A Review of Current Management Strategies. J Am Acad Orthop Surg. 2020;28(15)–e673.
Mollon B, et al. Arthroscopic vs. Open Synovectomy in PVNS: A Meta-Analysis. J Bone Joint Surg Am. 2015;97(6):522–534.
Murphey MD, et al. Imaging of Pigmented Villonodular Synovitis and Tenosynovial Giant Cell Tumor. Radiographics. 2008;28(5):1493–1518.
MRI Findings Summary Table
Feature | Description | Diagnostic Value |
Synovial Thickening | Diffuse or nodular proliferation of synovium lining the joint capsule | Seen in both localized and diffuse PVNS |
Signal Intensity (T1) | Iso- to hypointense relative to muscle | Hemosiderin deposition lowers T1 signal |
Signal Intensity (T2) | Predominantly low due to hemosiderin, sometimes mixed with high areas (fibrosis vs inflammation) | “Dark on T2” pattern is characteristic |
Blooming Artifact | Signal drop on gradient-echo (GRE) sequences caused by magnetic susceptibility of hemosiderin | Pathognomonic for PVNS |
Contrast Enhancement | Strong enhancement of synovial tissue, absent in cystic or necrotic areas | Reflects active disease |
Bone Involvement | Cortical erosion, pressure remodeling, subchondral cysts | Indicates chronic or advanced disease |
Extra-Articular Extension | Seen in diffuse type (knee, hip, ankle) | Helps determine need for open approach |
Joint Effusion | Usually minimal to moderate, occasionally hemorrhagic | Supports diagnosis but non-specific |
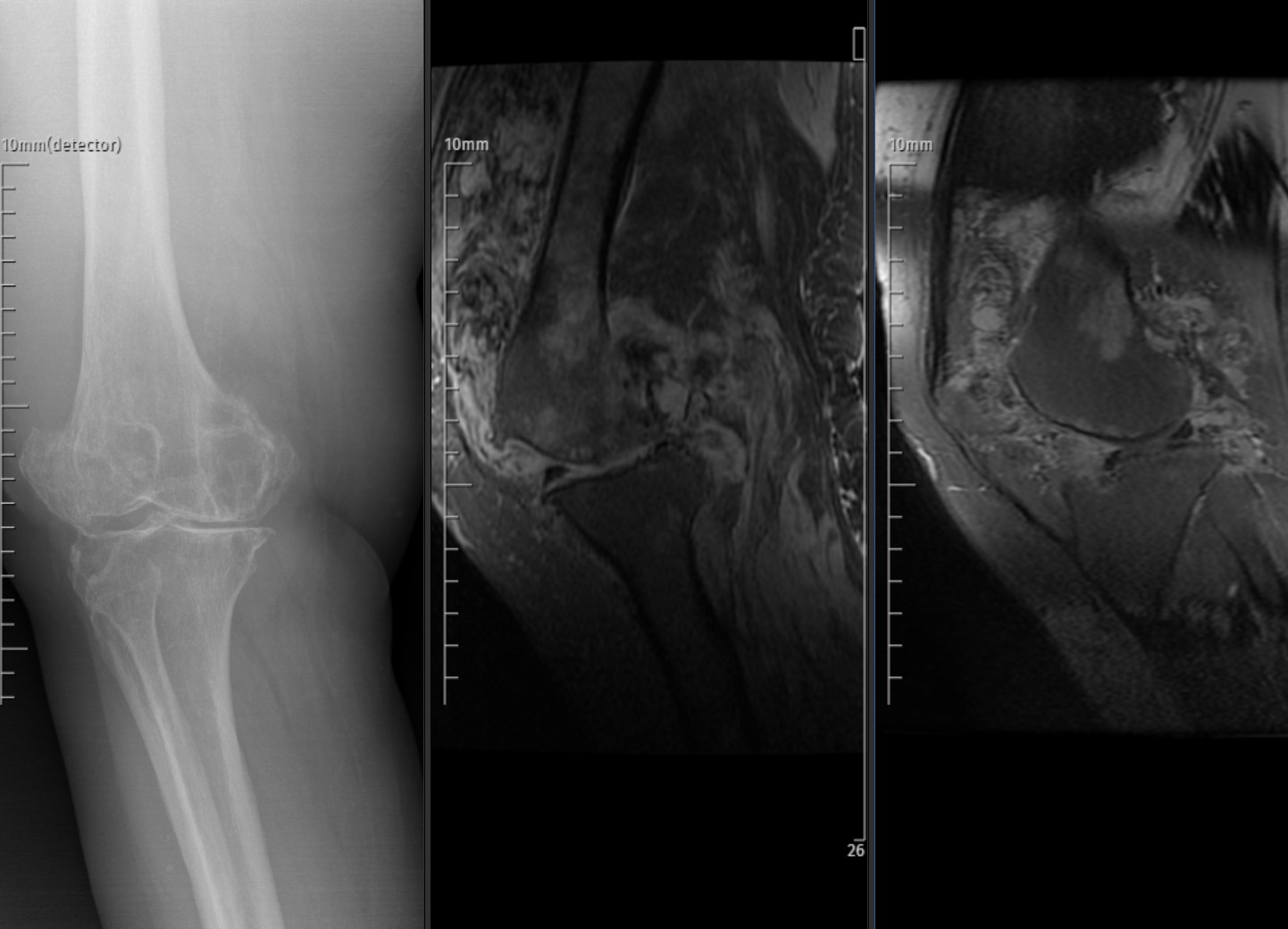
Radiograph and sagittal MRI images of the knee show diffuse synovial thickening with low-to-intermediate signal intensity and heterogeneous enhancement after contrast administration. Subchondral erosions and mild bone marrow edema are present. Findings are consistent with diffuse-type tenosynovial giant cell tumor (pigmented villonodular synovitis).
Pigmented villonodular synovitis
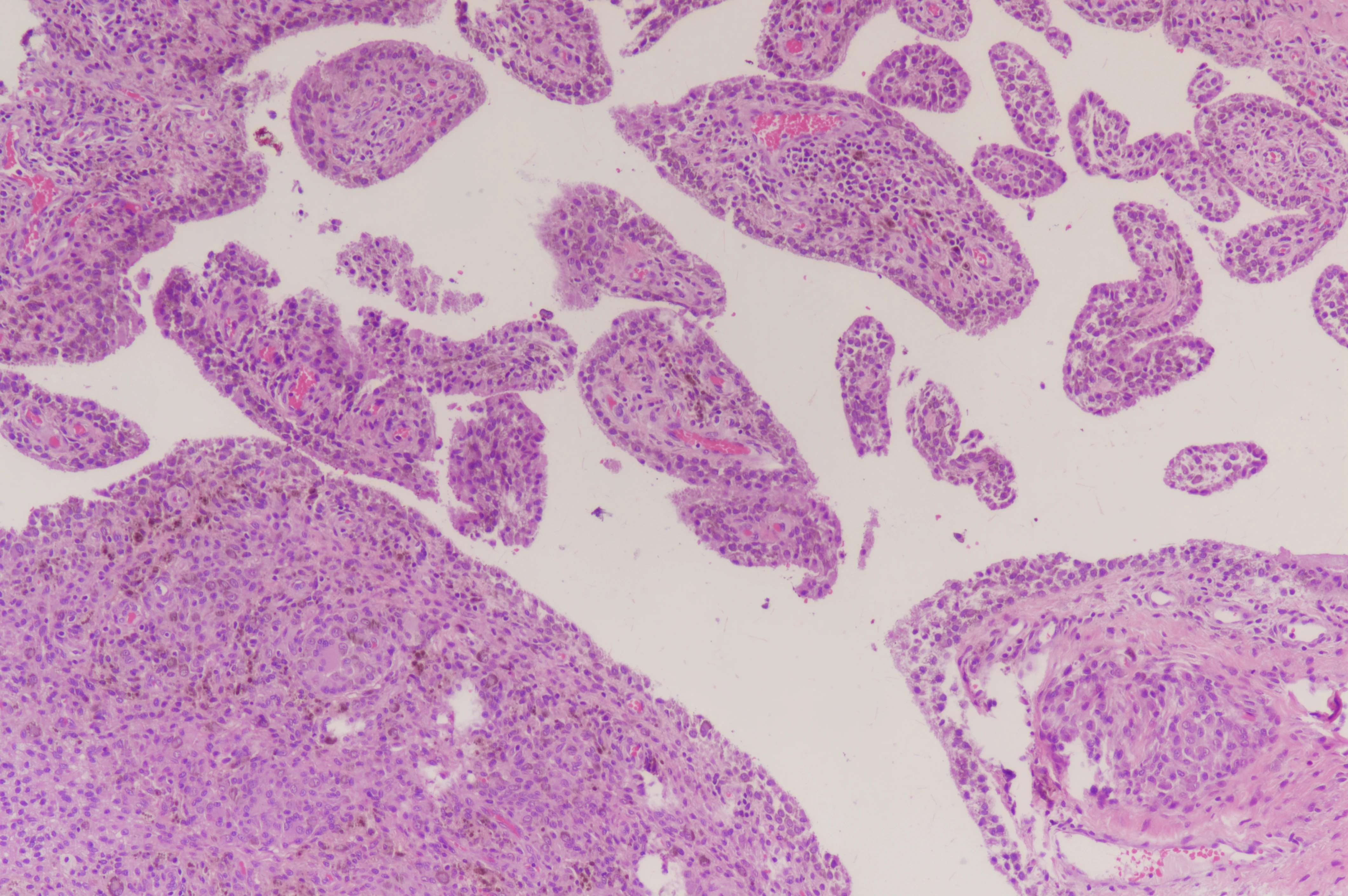
Tendon sheath tumor pathology
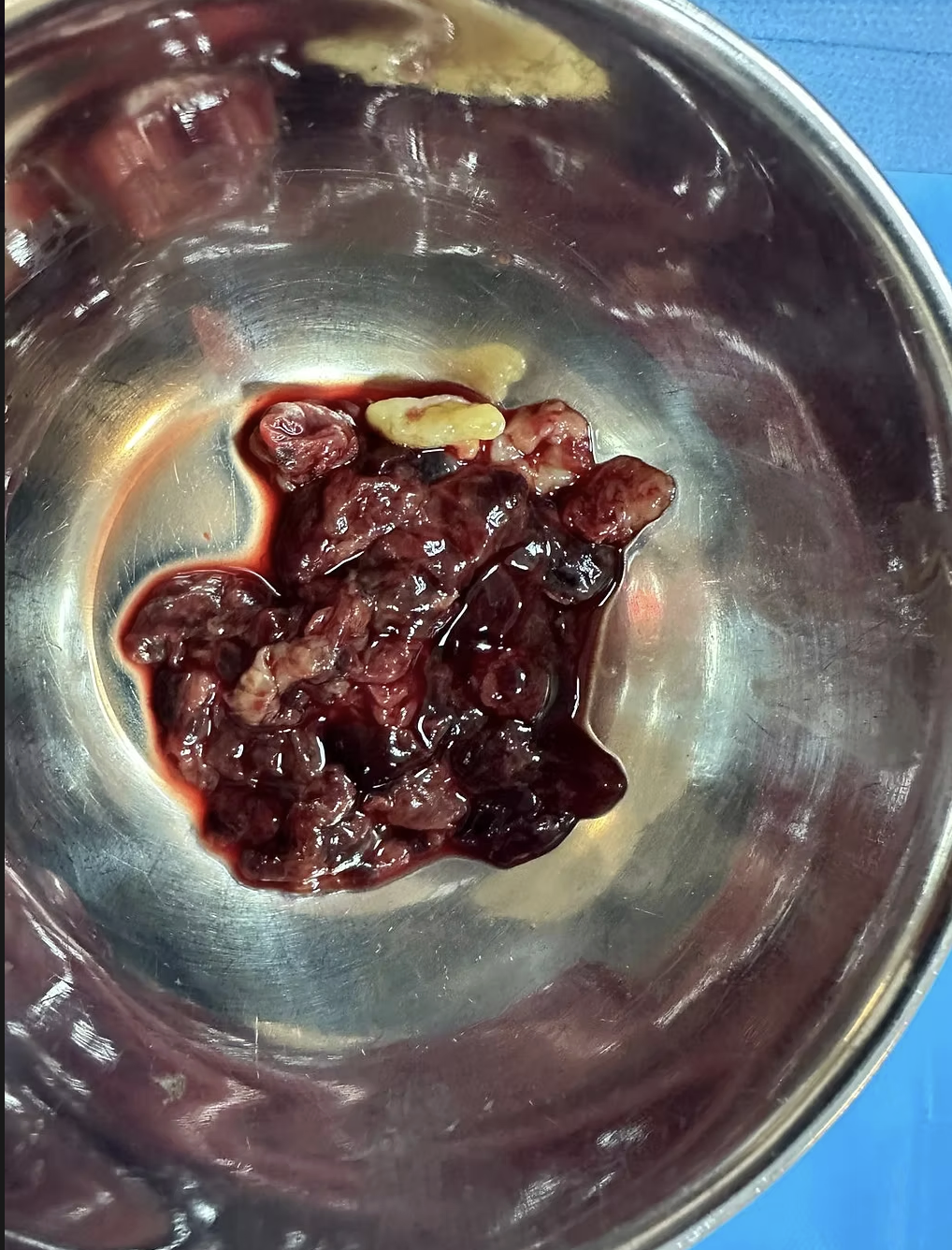
Peroperative mass from pvns