Epidemiology
The most common type of injured ligament in the knee
Accounts for 50% or more of all knee injuries 1**
In the United States, 250,000 people sustain ACL injuries each year.
2-10 times higher in female sports players, compared to males.
Tearing of these fibers can lead to instability of the knee, particularly anterolateral rotational instability, which can be manifested by giving way during heavy exercises, involving jumping, tackling, or twisting movements (e.g., soccer, field field hockey, and basketball).
Anatomy
The length 27 to 38 mm and the width 10 to 12 mm. The midsubstance cross-section area measures 44 mm². 3**
Extrasynovial ligament
Have two parts: the anteromedial (AM) and posterolateral (PL) bundles.
AM bundle, restrictor in forward translation; the PL bundle restrictor on tibial internal rotation.
The nerve supply; posterior articular branches of the tibial nerve.
The primary blood supply ; middle genicular artery.
Mechanism
Non-contact (%88), contact-direct, and contact-indirect mechanisms. 4**
the most common mechanism; sudden pivoting of the knee, prior contact, slight hip and knee flexion, and heel strike leading to valgus failure with neutral rotation of the knee such as soccer, field hockey, and basketball.
Presentation
Patient may hear a pop or feel a snapping sensation, effusion.
Feels abnormality (instability) in knee control.
Partial ACL tears, signs of instability may not develop.
Thirty-nine percent of partial ACL injury develop a complete tear, and half of the patients develop an accompanying meniscal lesion.
Diagnosis
Physical Exam
The Lachman test;
Demonstrates anterior translation. Should be done by comparing with the other knee.
Performed with the knee in extension and tests the posterolateral bundle by measuring the resistance of the tibia to forward translation. More than 5 mm of tibia protrusion compared to the opposite extremity and no hard resistance is encountered indicates ligament damage.
The pivot shift
Gives more accurate results, when performed under anesthesia.
Sudden subluxation movement occurring at 20°–30° flexion (with the displacement of the ITB posterior to the knee rotation center) in the knee joint brought from extension to flexion indicates that the test is positive.In the “IKDC (The International Knee Documentation Committee) classification”, instability is divided into four as “Grade 0 (normal), “Grade 1” (glide), “Grade 2 (clunk), “Grade 3” (locked subluxation).
Lever test
supine position, the examiner places their fist under the patient's calf and then presses the thigh against the table, just above the knee. In patients with a torn ACL, the heel remains in contact with the table.
Anterior drawer test
performed with the hip flexed at 45° and the knee flexed at 90°.Movement greater than 6–8 mm relative to the healthy knee is considered positive.Before performing, ensure that the posterior cruciate ligament is intact.With the knee flexed, resistance to anterior translation of the tibia is provided by the anterior medial bundle.
KT-2000, Telos and GNRB arthrometer are devices that measure instability numerically.
Imaging
Xray
useful in revealing fractures, evaluating varus and tibial slope
Eminentia fracture, a sign of ACL tear.
Segond fracture is associated with the anterolateral ligament (ALL).
MRI
The normal linear appearance of the ligament is replaced by an amorphous, high-signal tissue, with the ligament fibers losing continuity in their parallel course to the intercondylar notch.
Ripple at the anterior margin of the ACL in sagittal slices, high signal on T2-weighted images, and disruption in the continuity of the ACL.
Secondary findings; hemarthrosis, angulation of the posterior cruciate ligament, incomplete coverage of the posterior horn of the lateral meniscus by the condyle, areas of translational edema in the lateral compartment bones, and anterior position of the tibia.
“coronal oblique" and "sagittal oblique" positions for partial ACL injuries.
Identifies associated injuries; meniscal tears, lateral collateral ligament tears, posterolateral corner tears, and ALL injuries
In chronic tears, the horizontal orientation of hypointense remnant fibers and a gap may be observed in the intercondylar notch
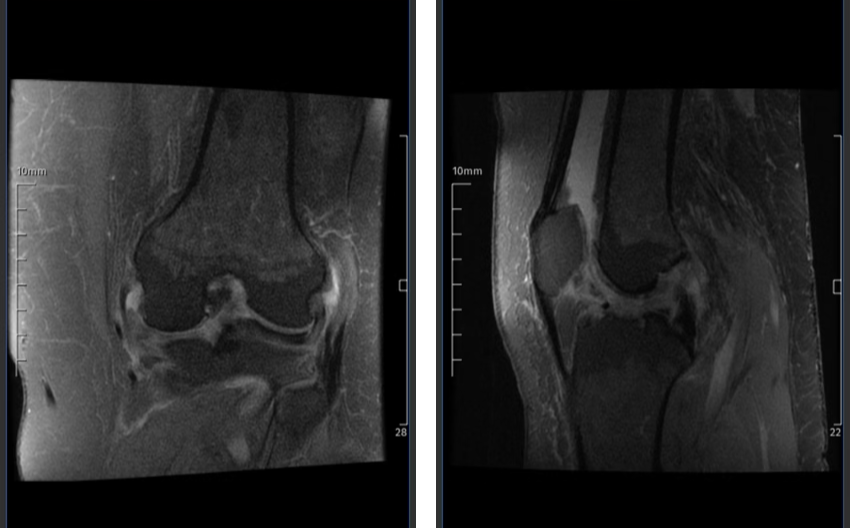
Anterior cruciate ligament rupture MRI
CT
Identifies segond fractures, avulsion fractures, osteochondral damage, and tunnel size before revision.
TREATMENT
In the early period
Resting with a compression bandage, ice and anti-inflammatory treatment.
Range of motion and quadriceps strengthening exercises
Surgical treatment
Arthroscopic reconstruction
Anatomical placement of grafts
Various autologous grafts, including grafts of the patellar tendon (BPTB), quadriceps tendon, peroneal tendon and hamstring tendon (semitendinosus and/or gracilis), as well as allografts and synthetic grafts
Graft selection should be based on the age, anatomy, requirements, and expectations of the patient.
Meniscus injuries are the most common pathologies accompanying ACL injuries..The results of meniscus repair are quite successful.Menisci should be preserved as much as possible and repair should be considered as a priority.
Surgery timing
Early reconstruction (surgery within 3 months) is not associated with improved functional outcomes nor fewer complications5**Top performers are immediate candidates for surgical intervention.
Surgical treatment is recommended when the acute inflammation and painful period is over and full range of motion in the knee joint and quadriceps muscle control is gained.
Treatment of partial tears
Augmentation, selective bundle reconstruction, and thermal modification options can be considered.
After ACL reconstruction, a gradual process of proliferation of synovial tissue and vascularization of tendons, defined as ‘’ligamentization,’’The graft has been shown to undergo an early phase of vascularization with rapid attenuation, followed by cellular development and maturation, which is completed approximately six months after graft placement and nearly transforms into the biological nature of the ligament.
Double-bundle graft to replicate a more physiologic function of ACL and to provide greater biomechanical stability 6**
Femoral tunnel
For the reconstruction of a single ligament, the optional position is in the center of the femoral and tibial origin
Surgical bony landmarks:
Lateral intercondylar ridge (resident’s ridge),defines the anterior margin of the femoral ACL insertion. 7**8**.
The bifurcate ridge demarcates the anterolateral and posteromedial bundles.
The femoral tunnel can be drilled with an anteromedial approach and a transtibial approach.
With the AM approach, the femoral tunnel is drilled through the anteromedial portal, while the knee is in maximum flexion between 125° and 130°.
With the transtibial technique, the femoral tunnel is drilled through the tibial tunnel.
The transtibial approach recreates a femoral tunnel more vertically on the coronal plane, this technique has a residual pivot shift and has a worse outcome compared to the anteromedial portal.
Tibial tunnel
Oriented parallel to the Blumensaat line on sagittal images on MRI or at lateral radiograph.
Place it lateral to the medial intercondylar process, just posterior to the anterior horn of the lateral meniscus, close to the direct fibers located within the ACL footprint.
Graft types selection
Autograft, allograft and synthetic grafts.
Autograft
Hamstring tendons, patellar tendon, quadriceps tendon, peroneal tendon, and iliotibial band.
Soft tissue grafts may take up to six weeks longer to adapt to the tunnel than bony tendon grafts.
Allograft
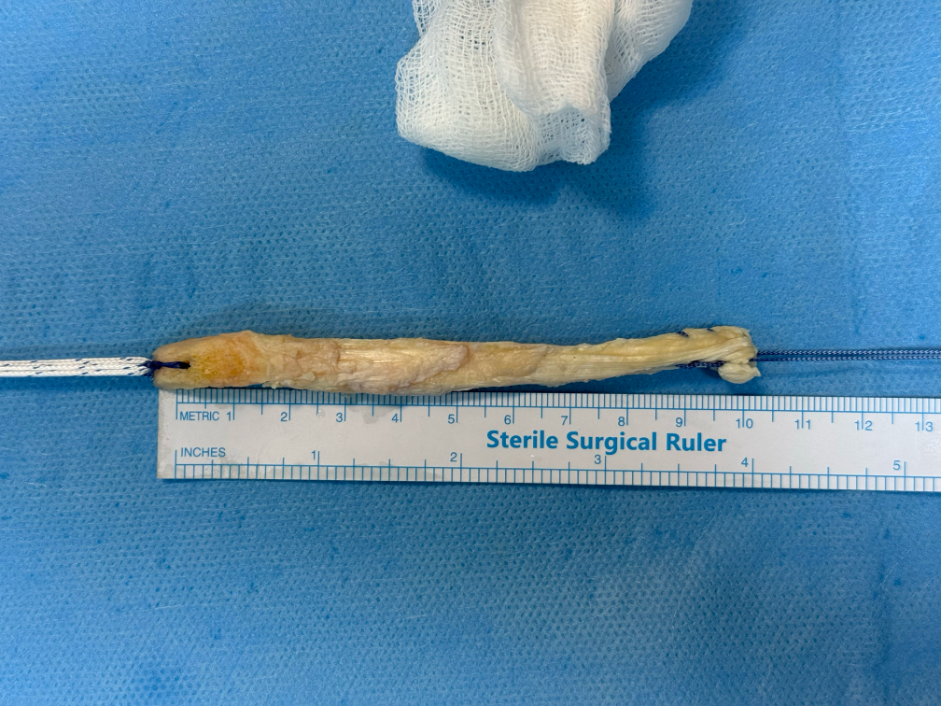
Tibialis posterior tendon, Achilles tendon, tibialis anterior tendon, bone-patellar tendon-bone and peroneus longus tendon.

Peroneus longus graft harvest
Hamstring graft;
The most widely used graft.Single or double-band, both semitendinosus and gracilis tendons or only the semitendinosus tendon.
Low donor site morbidity and kneeling is not seen.Lack of flexion strength and sensory deficit due to injury to the infrapatellar and sartorial branches of the saphenous nerve.
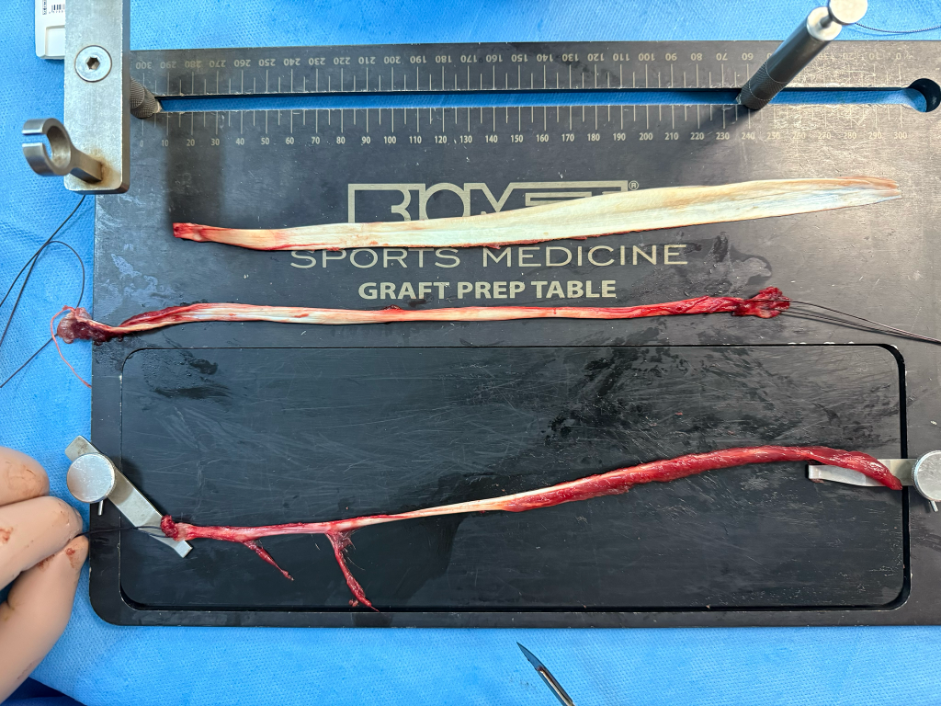
Peroneal tendon, gracilis and semitendinosus tendon
Bone-patellar tendon-bone
High durability and hardness, faster and easier adaptation to the tunnel. Disadvantages include kneeling pain, decreased knee extension strength, patella fracture, and patellar tendon rupture.
Quadriceps Autograft
Mini incision, it causes less anterior knee pain, does not reduce flexion strength, can be prepared with bone
Requires special instruments or meticulous surgical technique.
The modulus of the graft was found to be more similar to the anterior cruciate ligament.
Quadriceps tendon graft with bone block
Iliotibial band
Commonly used in pediatric anterior cruciate ligament and anterolateral ligament surgery.
Allografts
Absence of donor site morbidity, the availability of graft sizes in desired sizes, shorter surgery time, and ease of use in multiple ligament and revision surgeries.
Disadvantages include higher revision rates. Require a longer and weaker tunnel adaptation and remodeling process, and are biomechanically less durable.
Potential risk of immunological reactions, disease transmission, and the larger financial budget requirements
Fixation technique
Three groups of materials; intratunnel, extratunnel and suspension (cortical button), depending on where the graft is fixed.
"Bungee effect", the longitudinal movement of the graft within the tunnel
"Windshield wiper effect”, the horizontal movement of the graft within the tunnel.
The location of the graft fixation at the tunnel entrance or outside the tunnel is not statistically significant in terms of tunnel expansion, stability or functional results.
For anchorage of grafts interference screws, fixation devices such as endobutton or transfixation devices such as a cross-pin are used
Complications
Graft tear;
first cause of graft failure; most commonly due to a new injury
Can be partial or complete .
Partial graft tear, appears as a focal area of increased signal intensity on MR images, a complete graft tear is defined by the absence of intact fibers with an increased signal on T2-weighted sequences
Tunnel malposition and graft impingement
Femoral tunnel too anterior; may cause a tightened graft when the knee flexes, graft stretching and laxity of the graft on knee extended
Femoral tunnel too posterior; leads to a tightened graft in knee extension and laxity on flexion.
Roof impingement is the second cause of graft failure. The main cause of roof impingement is the too anterior positioning of the tibial fixation tunnel.
Tibial tunnel is positioned too far anteriorly, the graft comes into contact with the roof of the intercondylar notch during knee extension
The tibial tunnel is displaced too far laterally so the graft impinges on the sidewall of the intercondylar notch.
Tibial tunnel is too medially and vertically positioned, the graft comes into contact with the posterior cruciate ligament (PCL), limiting knee flexion
Anterior knee laxity
Due to postoperative thickening of the posterior capsule causing
Cystic degeneration of the graft
Late complication, also known as ganglion cyst formation, and may be responsible for pain and limitation of motion, but not related to graft failure.
Arthrofibrosis
Second cause of loss of terminal extension of the knee. The focal form, also known as ‘‘Cyclope lesion’’ because of its arthroscopic appearance, is a nodular lesion characterized by synovial hyperplasia and excessive production of fibro-proliferative tissue which may also contain osseous or cartilaginous tissue.
Typically localized on the anterior portion of the intercondylar notch, appearing on MRI as a well circumscribed nodule.
Partially torn ACL graft with fibers lying in the anterior intercondylar notch may mimic focal anterior arthrofibrosis on MRI, also called ‘‘Pseudocyclops lesion’’
Tunnel cyst
Can be associated with a widening of the tunnel
Septic arthritis
Rare complication, caused by Staphylococcus aureus.
Osteoarthritis
Risk factors for osteoarthritis seem to be meniscal injury, an interval more than 6 months from injury to reconstruction, and an age over 25 years at the time of surgery
Donor site abnormalities
More frequent when the patellar tendon is used
Device complications
Fracture of the device or/and intra- or extrarticular migration.
All support procedures
Provides further rotational stability and protection for the graft.
Beneficial in high-risk patients, e.g. patients with excessive laxity or malpositioning, younger patients, or when the surgery is a revision of the ACLR
ALL should be kept in mind in ACL injuries with high-degree pivot shift before surgery or residual pivot shift following anatomic reconstruction, in young active patients with underlying severe hyperlaxity, in athletes who will return to contact pivot sports, in the presence of Segond fractures, and in revision surgeries.
Anterolateral support procedures are performed in the form of traditional lateral extraarticular tenodesis and modern ALL reconstruction.
ACLR+anterolateral tenodesis significantly improved the rate of graft failure and return to sport, compared to ACLR in isolation. 9**.10**.
High tibial osteotomy
In patients with coronal plane deformities and associated low-medium-stage arthrosis, alignment should be corrected with concurrent high (proximal) tibial osteotomy in addition to ACL reconstruction
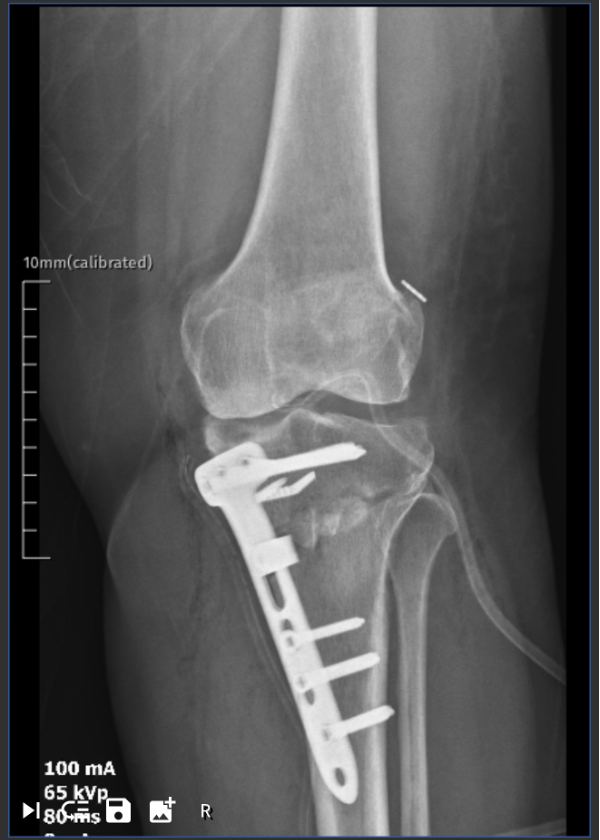
High tibial osteotomy combined anterior cruciate ligament reconstruction
Primary repair
In acute injuries near the femoral adhesion site, primary repairs can be performed by re-fixing the femoral adhesion site with high-strength suture material passed through the remnant connective tissue with the help of bone anchors or transosseous tunnels.
Four techniques have been described: dynamic intraligamentary stabilization (DIS) (Ligamys®), bridge-aided repair (BEAR), use of an internal brace, and refixation with a suture anchor.
Pediatric treatment
Adult-like transepiphyseal reconstructions can be applied to adolescents with Tanner Stage 4 and 5 development, while physis-preserving surgical reconstruction methods can be applied
Treatment options; High-quality rehabilitation alone (non-surgical treatment) or ACL reconstruction plus high-quality rehabilitation.
The current approach is to perform reconstruction without secondary cartilage and meniscus damage.
Dynamic, multijoint neuromuscular control is important. In young patients with an open physis and younger than 12 years, less importance is placed on muscular strength development and hypertrophy.
Conservative management
Rehabilitation is essential both before and after surgery.
Treatment option for middle-aged or elderly patients who have a sedentary lifestyle and will not return to sports activities, and for patients with chronic ACL insufficiency with advanced arthrosis.
Recommended to consider the activity level and the degenerative state of the joint rather than the age limit.
Three-phase program consisting of acute, recovery, and functional phases. The use of blood flow restriction, neuromuscular electrical stimulation, early lower limb training, neuromuscular and proprioceptive exercises, and psychosocial support have recently become popular modalities in ACLR rehabilitation. 11**12**
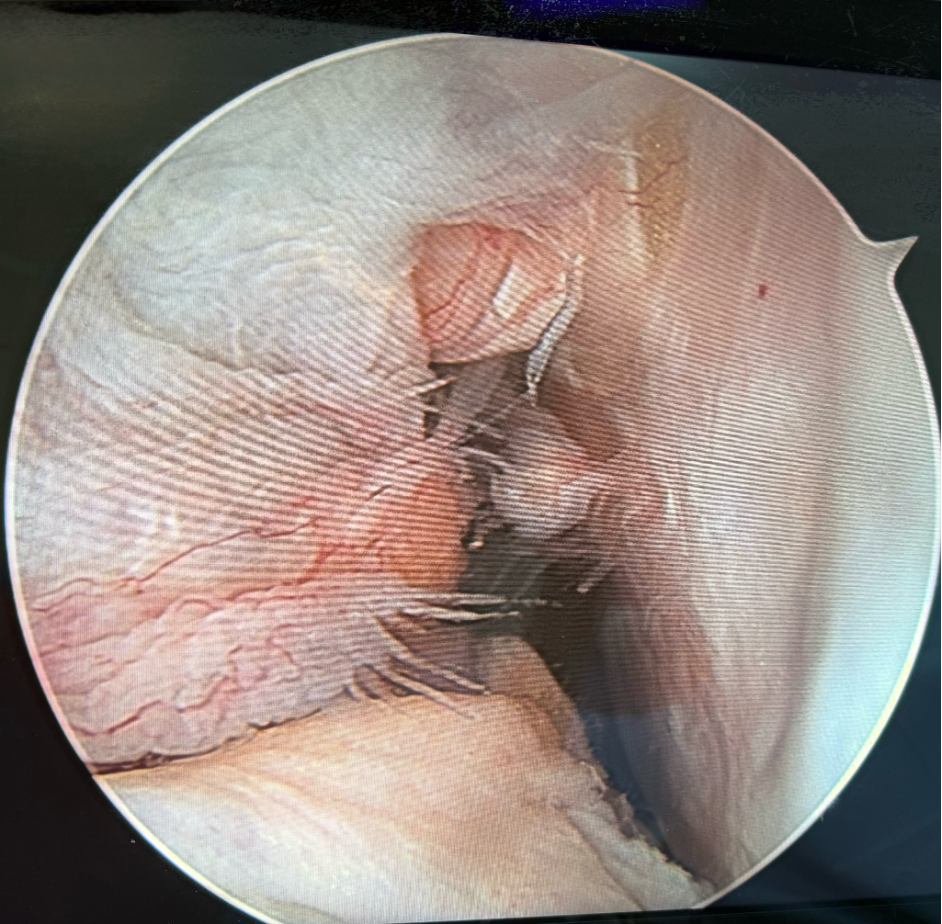
Torn anterior cruciate ligament arthroscopic diagnosis
Survey
86% of hamstring grafts used in ACLR generally survived 20 years.
In adolescents, this survival rate was 61%, dropping to 22% in those with a posterior tibial slope of 12° or more
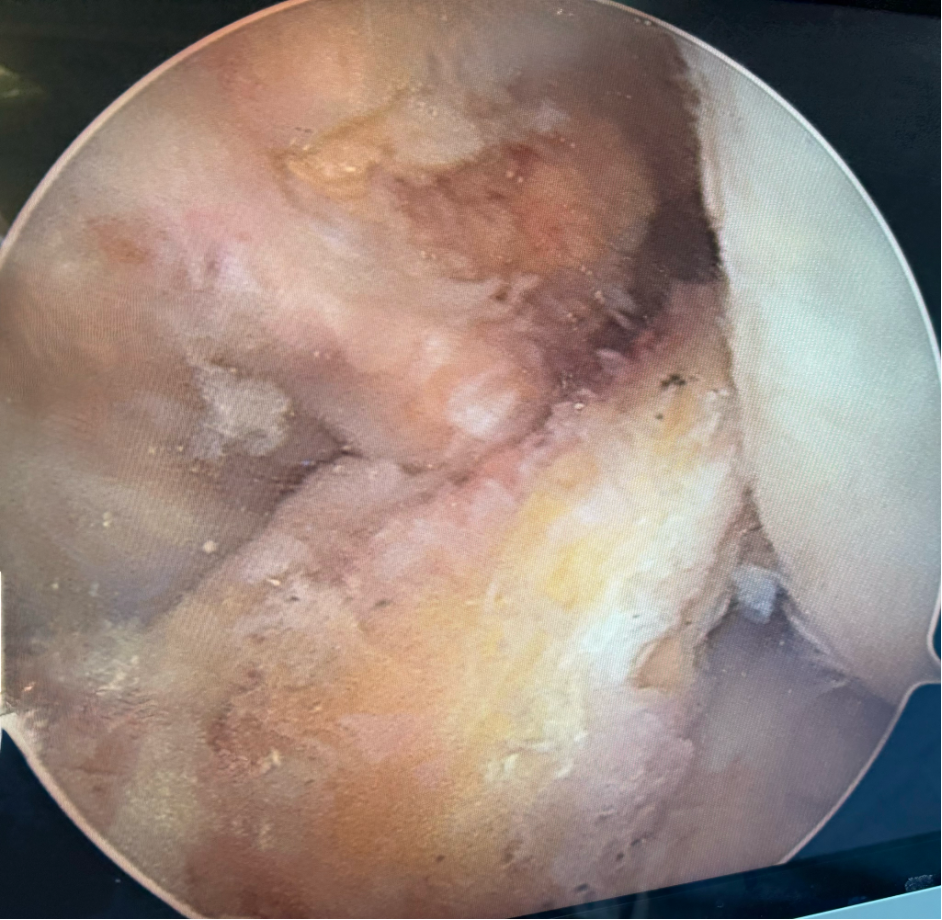
Appearance of the graft after acl reconstruction surgery
References:
Risberg MA, Lewek M, Snyder-Mackler L. A systematic review of evidence for anterior cruciate ligament rehabilitation: how much and what type? Physical Therapy in Sport. 2004; 5(3):125-145. doi:10.1016/j.ptsp.2004.02.003.
Mowbray MAS, Ireland J. Personal and narrative review of the current management of the injured anterior cruciate ligament of the knee in the UK with reference to surgical treatment versus rehabilitation. BMJ Open Sport Exerc Med. 2022; 8(3):e001410. doi: 10.1136/bmjsem-2022-001410
Morales-Avalos R, Torres-González EM, Padilla-Medina JR, Monllau JC. ACL anatomy: Is there still something to learn?. Revista espanola de cirugia ortopedica y traumatologia. 2024 Jul 1;68(4):422-7.
Lucarno S, Zago M, Buckthorpe M, et al. Systematic video analysis of anterior cruciate ligament injuries in professional female soccer players. Am J Sports Med. 2021; 49(7):1794- 1802. doi: 10.1177/03635465211008169.
Optimal Timing of Anterior Cruciate Ligament Reconstruction in Patients With Anterior Cruciate Ligament Tear Xianyue Shen 1, Tong Liu 2, Shenghao Xu 2, Bo Chen 1, Xiongfeng Tang 1, 2,✉, Yanguo Qin 1,✉JAMA Netw Open. 2022 Nov 17;5(11):e2242742. doi: 10.1001/jamanetworkopen.2022.42742.
Kiekara T, Ja ¨rvela ¨ T, Huhtala H, Paakkala A (2012) MRI of double-bundle ACL reconstruction: evaluation of graft findings. Skelet Radiol 41:835–842. doi:10.1007/s00256-011-1285-1
Rayan F, Nanjayan SK, Quah C, Ramoutar D, Konan S, Haddad FS (2015) Review of evolution of tunnel position in anterior cruciate ligament reconstruction. World J Orthop 18(6):252 262. doi:10.5312/wjo.v6.i2.252
Ferretti M, Ekdahl M, Shen W, Fu FH (2007) Osseous landmarks of the femoral atachment of the anterior cruciate ligament: ananatomic study. Arthroscopy 2:1218–1225
Meynard P, Pelet H, Angelliaume A, et al. ACL reconstruction with lateral extra-articular tenodesis using a continuous graft: 10-year outcomes of 50 cases. Orthop Traumatol Surg Res. 2020; 106(5):929-935. doi:10.1016/j.otsr.2020.04.007.
Sonnery-Cottet B, Barbosa NC, Vieira TD, Saithna A. Clinical outcomes of extra-articular tenodesis/anterolateral reconstruction in the ACL injured knee. Knee Surg Sports Traumatol Arthrosc. 2018; 26:596-604. doi:10.1007/s00167- 017-4596-5.
Andrade R, Pereira R, van Cingel R, Staal JB, Espregueira- Mendes J. How should clinicians rehabilitate patients after ACL reconstruction? A systematic review of clinical practice guidelines (CPGs) with a focus on quality appraisal (AGREE II). Br J Sports Med. 2020; 54(9):512-519. doi:10.1136/bjsports- 2018-100310.
Jenkins SM, Guzman A, Gardner BB, et al. Rehabilitation after anterior cruciate ligament injury: Review of current literature and recommendations. Curr Rev Musculoskelet Med. 2022; 15(3):170-179. doi:10.1007/s12178-022-09752-9A slowed-down rehabilitation protocol should be implemented that takes into account a return to sports over 8–12 months or longer.