Iliotibial Band Friction Syndrome (ITBFS)
Summary
Iliotibial band friction syndrome is characterized by repetitive rubbing of the iliotibial band (ITB) over the lateral femoral condyle, leading to lateral knee pain associated with activity. Clinically, diagnosis relies on detecting ITB tightness using Ober’s test and tenderness over the lateral femoral condyle, often worsened during a single-leg squat. Management is primarily nonoperative, including rest, NSAIDs, and stretching of the ITB, quadriceps, and gluteal muscles. Surgery, such as ITB release, is rarely needed for persistent, chronic cases.
Epidemiology
ITBFS accounts for 2–15% of all knee overuse injuries, predominantly affecting runners, cyclists, and athletes involved in repetitive knee flexion-extension activities. Risk factors include abrupt training changes, inadequate footwear, anatomical variations (genu recurvatum, genu varum, limb length differences, excessive pronation), weak hip abductors, tight ITB, and biomechanical imbalances (quadriceps-hamstring strength disparity, increased landing forces, higher knee flexion angle at heel strike).
Etiology and Pathophysiology
Repetitive forward and backward motion of the ITB over the lateral femoral condyle at around 30° of knee flexion causes friction, tension, and inflammation. This may lead to bursitis or cyst formation in the lateral synovial recess and sometimes femoral condyle edema. ITB pathology is less common. Associated conditions include patellofemoral pain, medial compartment osteoarthritis, varus deformity, and greater trochanteric pain syndrome, which can alter ITB biomechanics.
Anatomy
The ITB arises as a continuation of the tensor fascia lata and inserts onto Gerdy’s tubercle(Figure -1). Innervation is via the superior gluteal nerve (L4–S1), with hip abductors acting as synergists.
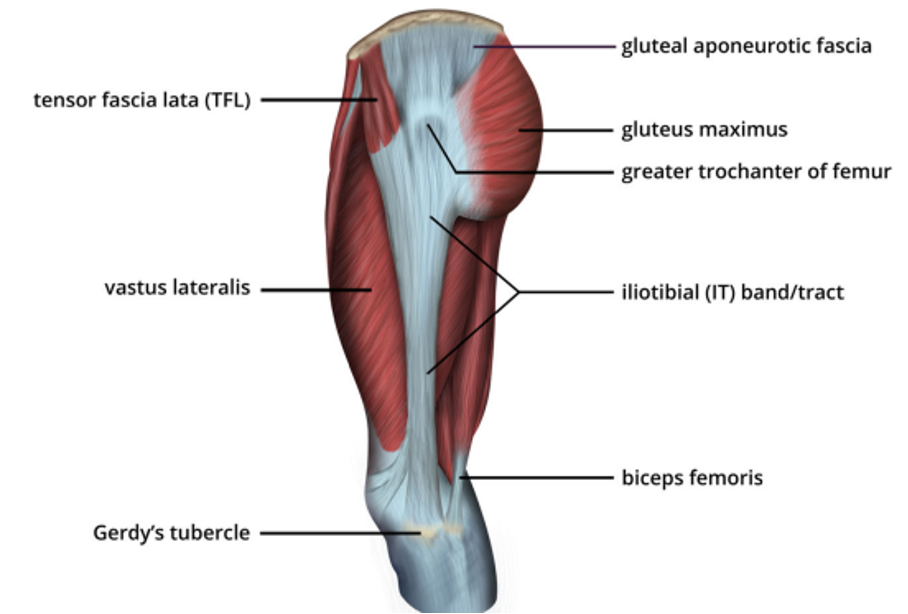
Figure-1 Illustration of the lateral view of the thigh demonstrating the iliotibial tract and important adjacent landmarks
Figure Reference
*Flato R, Passanante GJ, Skalski MR, Patel DB, White EA, Matcuk GR Jr. The iliotibial tract: imaging, anatomy, injuries, and other pathology. Skeletal Radiol. 2017;46(5):605-622. doi:10.1007/s00256-017-2604-y
Clinical Presentation
Patients report activity-related lateral knee pain, worsened by terrain or mileage changes. Examination may reveal lateral swelling, malalignment, tenderness over the lateral femoral condyle, crepitus, limited hip/knee motion, weak hip abduction, and pain reproduced on a single-leg squat or Ober test.
Imaging
X-rays (AP, lateral, oblique, skyline) are usually normal but may show bone changes or patellar malalignment. MRI is reserved for suspected associated soft-tissue injuries and may demonstrate signal changes in the lateral synovial recess, ITB, or periosteum.
Treatment
Nonoperative therapy is first-line: rest, ice, NSAIDs, corticosteroid injections, ITB and gluteal stretching, deep friction massage, hip abductor strengthening, proprioception exercises, and training adjustments. Surgery—arthroscopic or open excision of cysts/bursa, ITB Z-plasty, or elliptical band removal—is reserved for refractory cases.
Prognosis
Most patients (50–90%) improve within 4–8 weeks of conservative treatment.
Prepatellar bursitis
Prepatellar bursitis is inflammation of the bursa located over the front of the patella, often causing pain with kneeling(Figure-2). Clinically, it presents as anterior knee swelling, tenderness, and occasionally warmth, particularly in septic cases. Most cases are aseptic, but roughly 20% are caused by infection, with Staphylococcus aureus being the most common pathogen. Risk factors include repetitive kneeling, especially in wrestlers, who are also at higher risk for septic bursitis. Diagnosis is mainly clinical; aspiration with Gram stain and culture may be used if infection is suspected. Initial management is conservative, including compressive bandaging, NSAIDs, short-term immobilization, and selective aspiration. Corticosteroid injections are controversial. Surgical bursa excision, open or arthroscopic, is reserved for refractory or complicated cases.
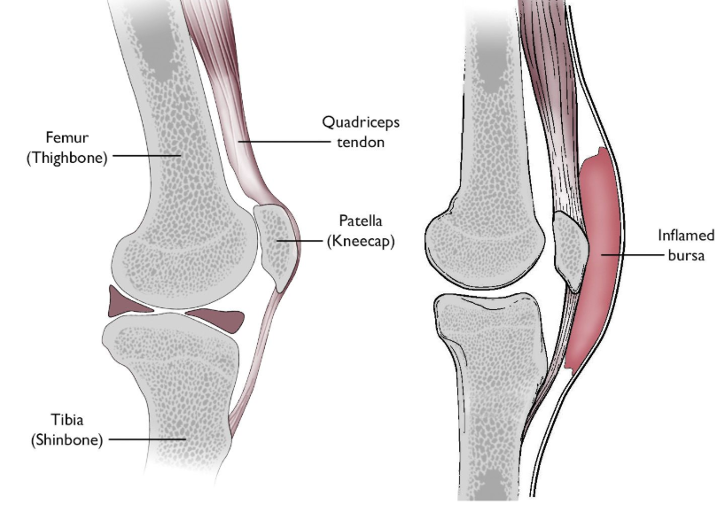
Figure-2 (Left) Normal knee anatomy shown from the side. The bursa is small and located between the patella and the skin. (Right) In prepatellar bursitis, the bursa becomes inflamed and swollen.
(Left) Reproduced from J Bernstein, ed: Musculoskeletal Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003. (Right) Reproduced and adapted from The Body Almanac. (c) American Academy of Orthopaedic Surgeons, 2003, p. 191.
Figure Reference : https://orthoinfo.aaos.org/en/diseases--conditions/prepatellar-kneecap-bursitis/
Quadriceps Tendonitis
Quadriceps tendonitis is inflammation of the quadriceps tendon at its attachment to the superior patella, typically causing anterior knee pain during activity.
Diagnosis is clinical, with tenderness at the tendon insertion and swelling; a palpable gap may indicate tendon rupture.
It primarily affects adult male athletes involved in jumping sports such as basketball, volleyball, or track events. Repetitive eccentric loading of the extensor mechanism causes microtears at the bone-tendon interface.
The quadriceps tendon is trilaminar, composed of rectus femoris (anterior), vastus medialis/lateralis (middle), and vastus intermedius (deep), innervated by femoral nerve branches.
Imaging is often normal; ultrasound can localize tendon damage, and MRI is the most sensitive.
Management is usually nonoperative, including rest, activity modification, NSAIDs, and physical therapy emphasizing quadriceps, hamstring, and core strengthening.
Corticosteroid injections are avoided. Surgery is rarely necessary and involves tendon debridement.
Patellar Tendinitis
Patellar tendinitis is a degenerative tendinopathy of the patellar tendon, commonly causing anterior knee pain related to activity. Diagnosis is primarily clinical, with tenderness at the distal pole of the patella in full extension. Basset’s sign—pain on palpation of the distal patella in extension but not in flexion—can help confirm the diagnosis. The condition mainly affects adolescent and young adult male athletes in jumping sports, especially volleyball, often associated with poor quadriceps and hamstring flexibility.
Blazina classification describes the severity of symptoms:
Phase I: Pain after activity only
Phase II: Pain during and after activity
Phase III: Persistent pain with or without activity, often impairing performance
Repetitive eccentric loading causes micro-tears and degeneration of the tendon. Imaging is often normal; chronic cases may show inferior traction spurs on X-ray, with ultrasound or MRI demonstrating tendon thickening and hypoechoic or hyperintense areas.
Treatment is primarily nonoperative, including rest, ice, activity modification, eccentric exercises, stretching, and supportive taping. Corticosteroids are contraindicated. Surgery—debridement and repair—is reserved for chronic Blazina stage III cases, with 80–90% return to sport.
* Strauss EJ, Kim S, Calcei JG, Park D. Iliotibial band syndrome: evaluation and management. J Am Acad Orthop Surg. 2011;19(12):728-736. doi:10.5435/00124635-201112000-00003
* Flato R, Passanante GJ, Skalski MR, Patel DB, White EA, Matcuk GR Jr. The iliotibial tract: imaging, anatomy, injuries, and other pathology. Skeletal Radiol. 2017;46(5):605-622. doi:10.1007/s00256-017-2604-y
* Baumbach SF, Lobo CM, Badyine I, Mutschler W, Kanz KG. Prepatellar and olecranon bursitis: literature review and development of a treatment algorithm. Arch Orthop Trauma Surg. 2014;134(3):359-370. doi:10.1007/s00402-013-1882-7
* Marigi EM, Buckley P, Razi F, et al. Patellar Tendinopathy: Critical Analysis Review of Current Nonoperative Treatments. JBJS Rev. 2022;10(3):e21.00168. Published 2022 Mar 8. doi:10.2106/JBJS.RVW.21.00168