Definition and Importance
SONK is a condition that can progress to end-stage knee arthritis.
After the hip, the knee is the second most common site for osteonecrosis.
As knowledge of its etiology and pathophysiology expands, treatment strategies continue to evolve.
Types of Knee Osteonecrosis[1,2,3,4]
Spontaneous Osteonecrosis (SONK)
The most frequent form of knee osteonecrosis.
Predominantly affects individuals over 50 years of age.
Reported incidence: 3.4% in those over 50, and 9.4% in those over 65.
Secondary Osteonecrosis
Occurs more often in younger patients.
Risk factors include sickle cell disease, myeloproliferative disorders, corticosteroid therapy, alcohol, and tobacco use.
Post-Arthroscopic Osteonecrosis
The rarest form.
Reported in about 4% of patients after knee arthroscopy, particularly following meniscus surgery.
Epidemiology[5,6,7]
Most common in women over 60 years old.
Usually unilateral.
More prevalent than secondary osteonecrosis but often remains unrecognized until advanced osteoarthritis develops.
More than 90% of cases involve the medial femoral condyle.
This predominance is associated with the limited vascular supply of the medial condyle.
Pathophysiology[5,6,7]
Historically attributed to ischemia-induced necrosis.
Current understanding: subchondral insufficiency fractures in osteopenic bone are the primary trigger.
Sequence: insufficiency fracture → bone marrow fluid accumulation → edema → focal ischemia → secondary necrosis.
A significant association exists between SONK and low bone mineral density in women over 60.
Clinical Presentation [5,6,7]
Symptoms
Sudden onset of medial knee pain without trauma.
Pain worsens at night, with walking, and during weight-bearing.
Physical Examination
Localized tenderness over the medial femoral condyle.
Frequently mistaken for medial meniscus tears during initial evaluation.
Classification[12]
Stage I: Knee symptoms but normal radiographs.
Stage II: Subchondral radiolucency with surrounding osteosclerosis and condylar flattening.
Stage III: Expansion of radiolucency and subchondral collapse.
Stage IV: Degenerative stage with osteosclerosis and osteophyte formation.
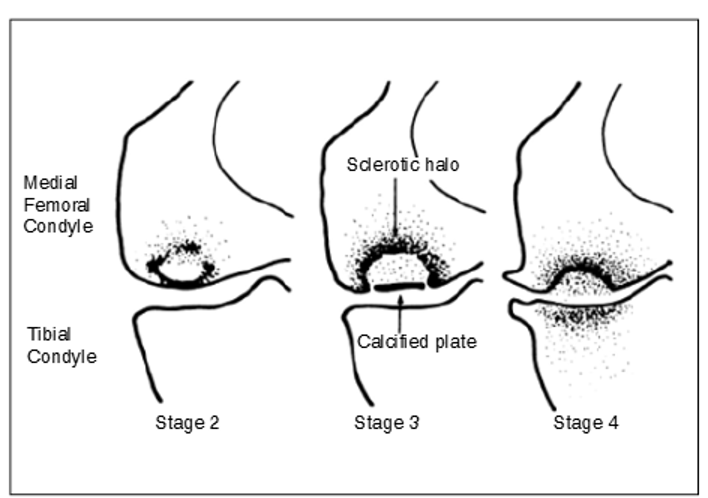
Figure 1:Koshino classification
Imaging [9,10,11]
Radiography
Initial assessment with AP, lateral, and oblique views.
Negative in early disease.
Late findings: condylar flattening or radiolucency.
Magnetic Resonance Imaging (MRI)
The most sensitive method for early diagnosis.
Typical findings: low signal intensity subchondral areas on T2, focal depressions of the epiphyseal contour, and low-signal lines within the condyle.
Bone Scintigraphy
May demonstrate increased uptake in the affected condyle.
Less sensitive and specific than MRI, not recommended for routine diagnosis.
Treatment [13]
General Principles
Treatment depends on symptom severity and lesion size.
Lesion dimensions measured on AP (width) and lateral (length) radiographs.
Lesion Size and Outcomes
Small lesions (<3.5 cm²): Often resolve with conservative management.
Medium lesions (3.5–5.0 cm²): Variable prognosis, may regress or progress.
Large lesions (>5.0 cm²): Usually progress to condylar collapse, requiring surgical intervention.
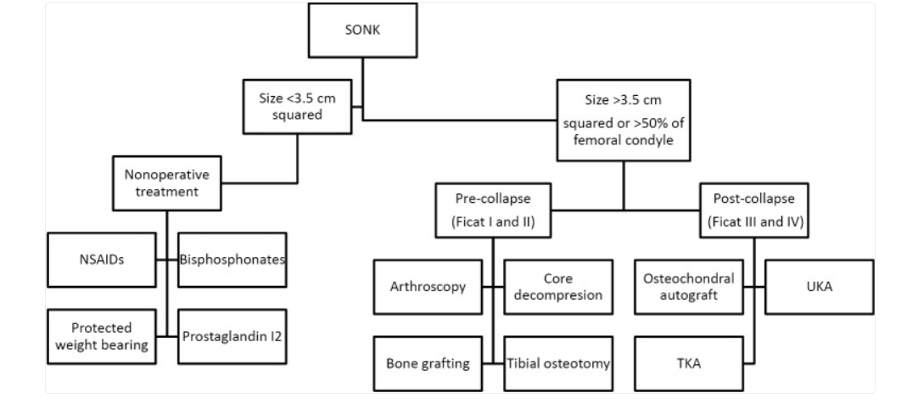
Figure 2: Treatment Algorithm
References
1. Cetik O, Cift H, Comert B, et al. Risk of osteonecrosis of the femoral condyle after arthroscopic chondroplasty using radiofrequency: a prospective clinical series. Knee Surg Sports Traumatol Arthrosc 2009;17:24-9
2. Pape D, Seil R, Fritsch E, et al. Prevalence of spontaneous osteonecrosis of the medial femoral condyle in elderly patients. Knee Surg Sports Traumatol Arthrosc 2002;10:233-40
3. Mont MA, Marker DR, Zywiel MG, et al. Osteonecrosis of the knee and related conditions. J Am Acad Orthop Surg 2011;19:482-94
4. Mont MA, Baumgarten KM, Rifai A, et al. Atraumatic osteonecrosis of the knee. J Bone Joint Surg Am 2000;82:1279-90
5. Mears SC, McCarthy EF, Jones LC, et al. Characterization and pathological characteristics of spontaneous osteonecrosis of the knee. Iowa Orthop J 2009;29:38-42
6. Yamamoto T, Bullough PG. Spontaneous osteonecrosis of the knee: the result of subchondral insufficiency fracture. J Bone Joint Surg Am 2000;
7. .Akamatsu Y, Mitsugi N, Hayashi T, et al. Low bone mineral density is associated with the onset of spontaneous osteonecrosis of the knee. Acta Orthop 2012
8. Lotke PA, Abend JA, Ecker ML. The treatment of osteonecrosis of the medial femoral condyle. Clin Orthop Relat Res 1982;(171):109-16.
9. Fotiadou A, Karantanas A.Acute nontraumatic adult knee pain: the role of MR imaging. Radiol Med 2009;114:437-47
10. Mont MA, Ulrich SD, Seyler TM, et al. Bone scanning of limited value for diagnosis of symptomatic oligofocal and multifocal osteonecrosis. J Rheumatol 2008;35:1629-34.
11. Pivec R, Johnson AJ, Harwin SF, et al. Differentiation, diagnosis, and treatment of osteoarthritis, osteonecrosis, and rapidly progressive osteoarthritis. Orthopedics 2013;36:118-25.
12. Barroso, G. C., Fuchs, T., Thiele, E., & Lima, M. N. (2012). Osteonecrose espontânea do joelho em atleta tratamento com o uso de câmara hiperbárica: relato de caso e revisão de literatura. Revista Brasileira de Ortopedia, 47, 389-393.
13. Karim, A. R., Cherian, J. J., Jauregui, J. J., Pierce, T., & Mont, M. A. (2015). Osteonecrosis of the knee. Annals of translational medicine, 3(1), 6.