Figures
1.Definition and Overview
Brachial plexus injuries involve the C5–T1 nerves , resulting in varying degrees of motor deficit, sensory loss, and functional impairment of the upper limb.
2. Etiology
Traumatic (Most Common): Generally occurs following high-energy trauma or traction injuries (e.g., motorcycle accidents, work accident, falling from a height, gun shot wounds, stub injuries) , tumors ( local or metastatic), radiotheraphy, iatrogenic surgical complications.
Obstetric: Birth-related injuries.
3.Anatomy
Roots → Trunks → Divisions → Cords → Branches
Supraclavicular region (roots and trunks) or infraclavicular region or both
4. Classification
A. By Level:
Upper Plexus (C5–C6) - Erb’s Palsy: Characterized by the loss of shoulder abduction and elbow flexion.
Intermediate (C567)
Lower Plexus (C8–T1) - Klumpke Palsy: Presents with hand weakness. Possible Horner syndrome.
Total Plexus Injury: Paralysis of the entire arm (flail limb).
B. By Severity:
Neuropraxia: Temporary conduction block; full recovery is expected.
Axonotmesis: Axonal damage is present, but the nerve sheath remains intact; recovery is possible.
Neurotmesis: Complete disruption of the nerve, no recovery expected, requires surgical intervention.
C. Pre-ganglionic vs. Post-ganglionic:
Preganglionic (Root Avulsion): Traction rupture of the nerve root from the spinal cord. It has the worst prognosis as no direct repair is possible. Horner sign in Klumpke palsy
Postganglionic (Rupture): Offers better surgical options and outcomes.
5. Clinical Presentation & Red Flags
Clinical presentation includes weakness or paralysis, sensory deficits, and neuropathic pain especially in traumatic injuries.
Red Flags:
Flail limb
Severe, intractable pain
Horner syndrome (indicates root avulsion C8T1)
6. Diagnosis and Imaging
Physical Examination: Motor testing of key muscle groups, sensory mapping, and reflex evaluation, Horner sign.
Imaging: MRI Neurography is used to visualize root avulsions, nerve injury and injury level, and soft tissue injuries. CT Myelography can also be used for detecting root avulsions. Xray and CT for accompanying fractures
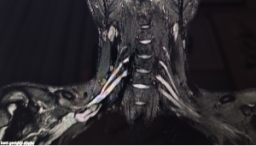
Figue 1: MR Neurography is a very helpful for imaging brachial plexus injury
EMG / NCS: Essential for functional assessment and nerve conduction status and for follow up.
7. Treatment Management
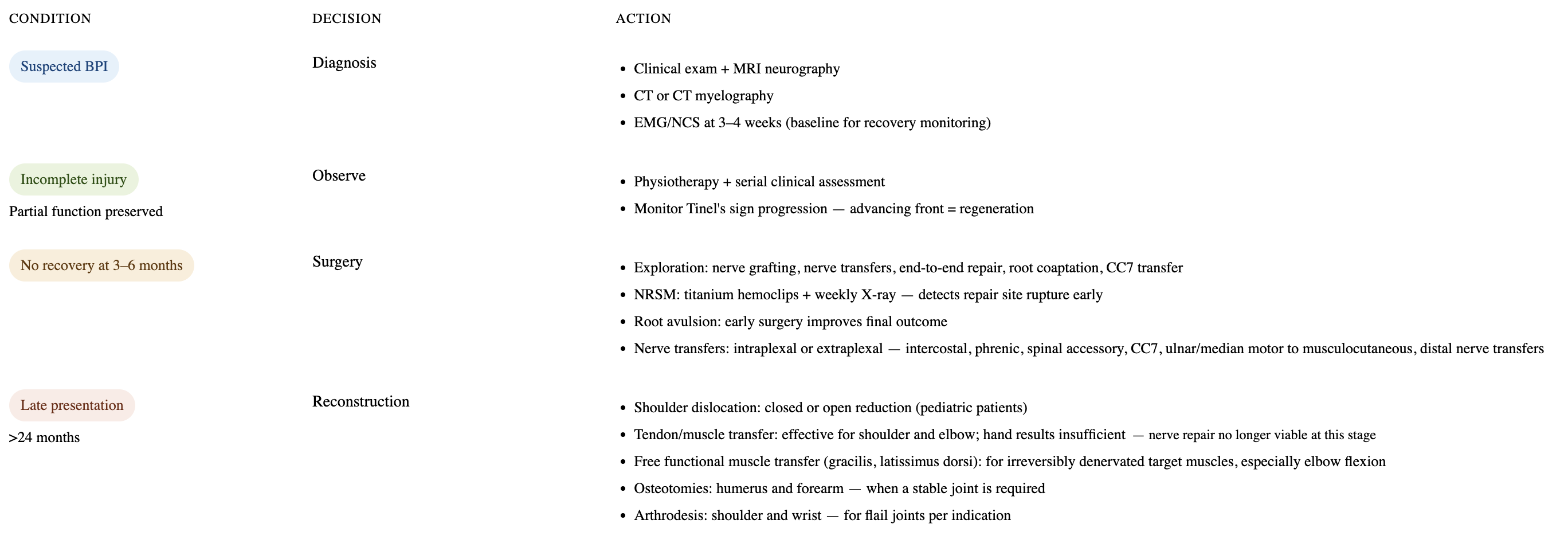
A. Nonoperative Treatment: Indicated for neuropraxia and early injuries (<3 months). Managed with physiotherapy, splinting, and close observation.
B. Operative Treatment & Current Approaches:
Timing (Critical): Surgery is indicated if there is no recovery at 3–6 months, or early surgical repair if there is open injury or a complete injury/root avulsion is diagnosed. Delayed surgery after 6 months leads to a worse prognosis.
Surgical Options: Nerve grafting, End to End repair, nerve transfers intraplexal or extraplexal donor (e.g., spinal accessory to suprascapular nerve; intercostal to musculocutaneous nerve), and for late cases, tendon or free functional muscle transfers, osteotomies, arthrodesis.
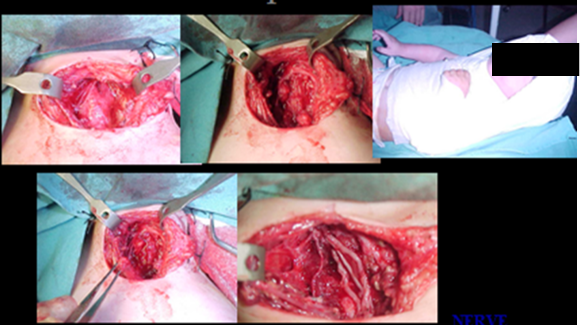
Figure 2: Exploration of brachial plexus. Erb neuroma excision and sural nerve grafting.
End-to-End Repair & The NRSM Technique (Pits & Pearls) End-to-end nerve repair is considered the ideal method for nerve reconstruction because it reduces the number of repair zones and shortens the distance to the target organ, providing earlier innervation. Clavicle osteotomy and 4 cm humeral shorthening can be done in traumatic patients. Figure 1: However, the greatest risk in end-to-end repair is nerve rupture at the repair site due to slight tension or ischemia. Detecting a rupture at the brachial plexus region is highly difficult because conventional modalities like high-resolution ultrasound, MRI, and diffusion tensor imaging (DTI) are insufficient for monitoring in this area.

Figure 3: Traumatic brachial plexus closed injury. C7, C8, T1 root avulsion. Clavicle osteotomy done for nerves disections and mobilizations. 4 cm humeral shorthenning done for end-to-end nerve repair. Upper trunk sutured to C5 , lower trunk sutured to C6. NRSM hemoclips seen at the neck region. Plate and screw fiation of humerus and clavicle done.
To solve this, the NRSM (Nerve Repair Site Marking) by using titanium hemoclip technique proximal and distal epineurium of the repair site is a simple, highly reliable, safe, and cheap technique and follow-up done only by Xray.
How it is done: During surgery, small titanium hemoclips are attached to the epineurium at least 5 mm proximal and distal to the nerve repair site.
Figure 4: A-Iatrogenic lower trunk injury during endoscopic thoracic out let surgery. B- Clavicle osteotomy and end-to-end repair done 6 months later. C- NRSM hemoclips seen in the xray.
Follow-up: The integrity of the end-to-end nerve repair is followed simply by taking standard X-rays every week for 6 weeks postoperatively. To eliminate magnification errors caused by X-ray tube distance, a "coin technique" can be used where a coin is placed near the surgical site to easily calculate the magnification ratio.

Figure 5: Obstetric palsy end-to-end upper trunk repair. During follow-ups metal coin put to the operated area. Since we know the diameter of the coin we can ratio the magnification by measuring the coin diameter on the xray. So we can measure the real distance of NRSM. This method is very helpful when there is suspicion of rupture.
Clinical Significance: If the distance between the hemoclips increases on the X-ray, a repair site rupture is diagnosed, allowing the surgeon to perform immediate revision surgery in the early period. This method has no morbidity or side effects.
References
Yuceturk A. X-ray follow up of end-to-end nerve repair site: A new technique, nerve repair site marking (NRSM). Hand Microsurg. 2016;5(3):118-123.
Yücetürk S.A. Is it possible to follow the risk of rupture after end-to-end nerve repairs in brachial plexus surgery Technical note. Acta Orthop Traumatol Turc. 2023 May;57(3):120-123. doi: 10.5152/j.aott.2023.22157.
Howarth HM, Alaziz T, Nicolds B, O’Connor S, Shah SB. Redistribution of nerve strain enables end-to-end repair under tension without inhibiting nerve regeneration. Neural Regen Res. 2019;14(7):1280-1288
Bhatia A, Doshi P, Koul A, Shah V, Brown JM, Salama M. Contralateral C7 transfer: is direct repair really superior to grafting? Neurosurg Focus. 2017;43(1):E3.
Wang S, Yun YX. Contrlateral C7 nerve transfer with dirsect coaptation to restore lower trunk function after traumatic plexus avulsion injuries. J Bone Joint Surg, (Am.). 2013;95(9):821-827.
Liao WC, Chen JR, Wang YJ, Tseng GF. The efficacy of end-to-end nerve repair (neurorraphy) in the rat brachial plexus. J Anat. 2009;215(5):506-521.
Nassimizadeh MS, Nassimizadeh AK, Power D. Managing the nerve gap: new tools in the peripheral nerve repair toolbx. J Musculoskelet Surg Res. 2019;3(1):4-8.
Karabay N, Çetinkol E, Toros T. Peripheral nerve imaging techniques. In: Dahlin LB, Leblebicioğlu G, eds. Current Treatment of Nerve Injuries and Dis-orders. FESSH 2013 Intructional courses. Ankara: Palme publications; 2013:151-165.
Martín Noguerol T, Barousse R, Gómez Cabrera M, Socolovsky M, Bencardino JT, Luna A. Functional MR neurography in evaluation of peripheral nerve trauma and postsurgical assessment. RadioGraphics. 2019;39(2):427-446.
Luzhansky ID, Sudlow LC, Brogan DM, Wood MD, Berezin MY. Imaging in the repair of peripheral nerve injury. Nanomedicine (Lond). 2019;14(20):2659-2677.
Heep H, Xu J, Löchteken C, Wedemeyer C. A simple and convenient method guide to determine the magnification of digital X- rays for preoperative planning in total hip arthroplasty. Orthop Rev (Pavia). 2012;4(1):e12.