1. General Overview & Epidemiology
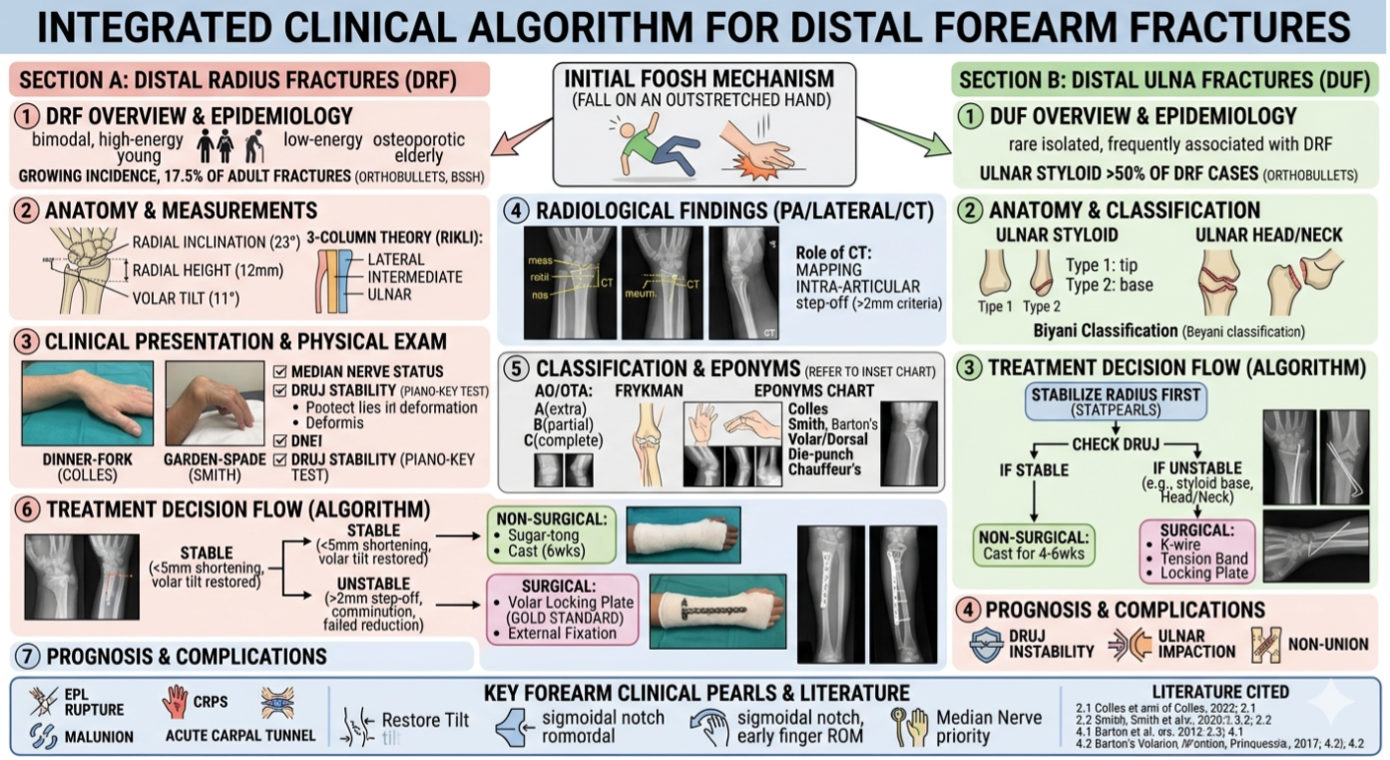
Distal Radius (DRF): Accounts for approximately 17.5% of all adult fractures.
Distribution: More common in females (2-3:1)
· Younger patients: High-energy trauma (sports, falls from height, motor vehicle accidents).
· Elderly patients: Low-energy falls (osteoporotic "fragility fractures").
Distal Ulna: Isolated fractures are rare (~5% of forearm fractures). Most occur in conjunction with a distal radius fracture, particularly ulnar styloid fractures (found in over 50% of DRFs).
2. Relevant Anatomy
· Anatomic location
Approximately 65% extra-articular, 10% partial articular, and 25% complete
· Risk factors
Osteoporosis (high incidence of distal radius fractures in women > 50 years old, distal radius fractures are a predictor of subsequent fractures)
DEXA scan is recommended for older patients with distal radius fractures and/or lower energy mechanisms
The distal radius and ulna together form the structural framework for wrist rotation (pronation/supination).
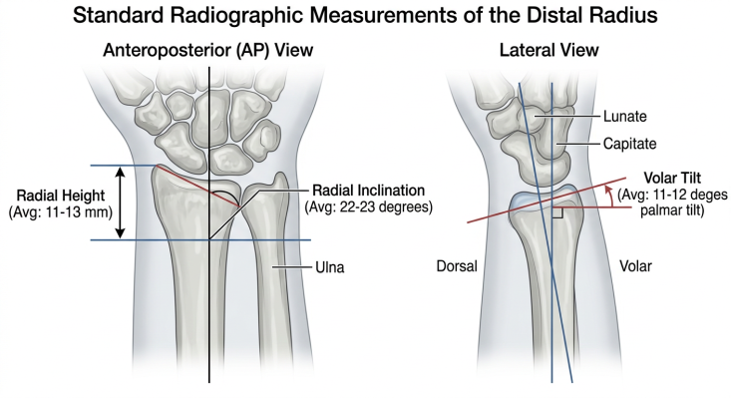
Radial Measurements (Normal):
Radial Inclination: Average 22–23°.
Radial Height: Average 11–12 mm.
Volar Tilt: Average 11–12°.
Column Theory (Rikli and Regazzoni):
Lateral Column: Radial styloid (attachment for brachioradialis).
Intermediate Column: Lunate fossa and sigmoid notch (load-bearing).
Medial Column: Distal ulna and TFCC (rotation axis).
TFCC (Triangular Fibrocartilage Complex): The primary stabilizer of the DRUJ.
Lister's Tubercle
On dorsal surface of distal radius, approximately 1 cm proximal to articular surface
EPL tendon lies just ulnar to tubercle before taking sharp turn into the thumb
Important landmark to avoid EPL attritional rupture with long volar plate screws
· Watershed region
Most volar and prominent aspect of distal Radius
Lunate portion is most prominent with vital short radiolunate ligament attachment for radiocarpal stability
Important region to remain proximal to for volar plate fixation
3. Clinical Presentation & Physical Examination
Symptoms: Severe pain, swelling, and localized tenderness. Deformities (Eponyms):
Name | Description | Mechanism / Clinical Note |
Colles' | Extra-articular; Dorsal angulation/displacement. | "Dinner-fork" deformity; most common fragility fracture. |
Smith's | Extra-articular; Volar angulation/displacement. | "Garden-spade" deformity; often more unstable than Colles'. |
Barton's (Volar) | Intra-articular fracture-dislocation; Volar lip involvement. | High risk of carpal subluxation; usually requires surgery. |
Barton's (Dorsal) | Intra-articular fracture-dislocation; Dorsal lip involvement. | Similar to Volar Barton's but involving the dorsal articular rim. |
Chauffeur's | Transverse/Oblique Radial Styloid fracture. | Also called "Backfire fracture"; often involves the scapholunate ligament. |
Die-punch | Depressed fracture of the Lunate Fossa. | Result of axial load through the lunate; causes articular incongruity. |
Physical Examination:
Neurovascular Status: Essential to check the Median Nerve (sensation in the thumb, index, and middle fingers) as acute Carpal Tunnel Syndrome is common.
DRUJ Stability: Palpate the distal ulna; look for "piano-key" instability (dorsal-volar translation).
Compartment Syndrome Check: Pain out of proportion or with passive finger extension.
4. Radiological Findings
Standard PA and Lateral X-rays are mandatory.
PA View: Assess radial inclination, height, and ulnar variance.
Lateral View: Assess volar tilt and "teardrop" angle.
Radiographic Criteria | Measurement (Normal) | Acceptable Reduction Criteria |
Radial Height (AP) | 13 mm | < 5 mm shortening |
Radial Inclination (AP) | 23° | Change < 5° |
Articular Stepoff (AP/Lat) | Congruous | < 2 mm stepoff |
Volar Tilt (Lateral) | 11° (Volar) | < 5° Dorsal angulation (or within 20° of contralateral side) |
CT Scan: Indicated for intra-articular fractures to map the fragments (e.g., "die-punch" fragment) for surgical planning.
MRI: Evaluate for soft tissue injury,TFCC injuries, scapholunate ligament injuries (DISI),lunotriquetral injuries (VISI)
5. Classification Systems
A. Distal Radius Classifications
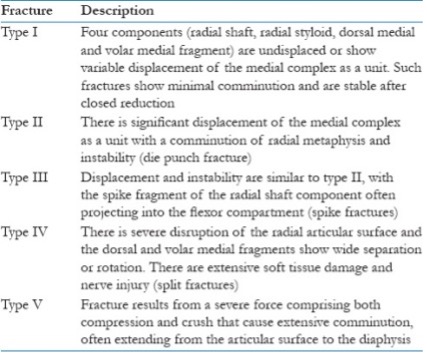
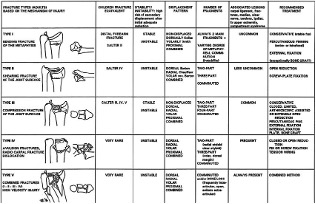
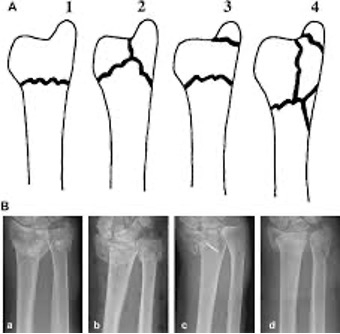
Melone :Divides intra-articular fractures into 4 types based on displacement
Fernandez: Bending, Compression (Intra-articular), Shearing (Barton), Avulsion, or Combined.
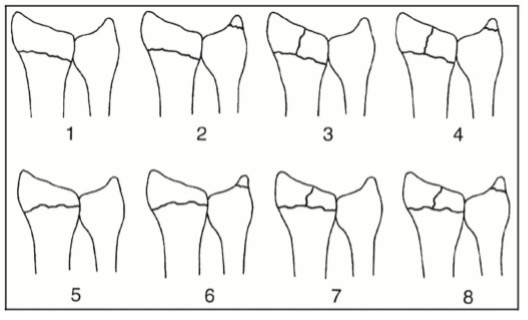
Frykman: Based on joint involvement (radiocarpal and/or radioulnar) +/- ulnar styloid fracture
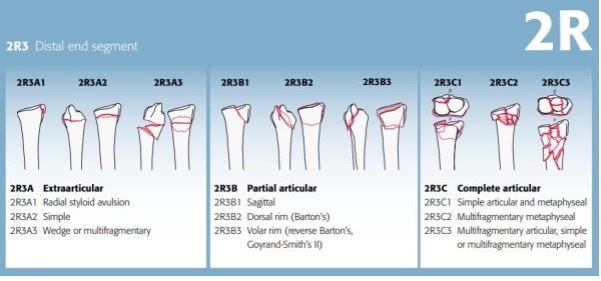
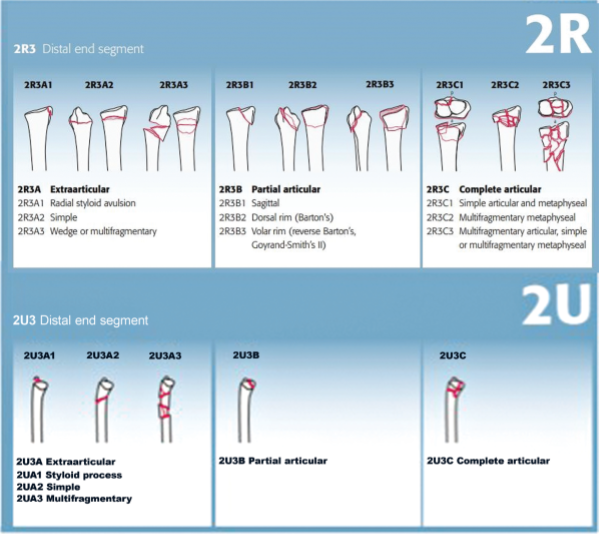
AO/OTA: comprehensive but cumbersom. Type A: Extra-articular; Type B: Partial intra-articular; Type C: Complete intra-articular.
B. Distal Ulna Classifications
Biyani Classification: Used for ulnar styloid fractures (Type 1: Non-articular; Type 2: Involves the base, affecting DRUJ stability).
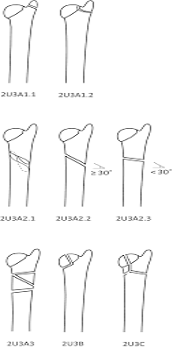
AO/OTA: Categorizes ulnar head and neck fractures separately.
6. Treatment Strategies
Non-Surgical (Conservative)
Indications: Nondisplaced or stable extra-articular fractures.
Management: Closed reduction followed by a Sugar-tong splint or Short-arm cast.
Surgical (Operative)
Indications: Failure to maintain reduction, intra-articular step-off >2mm, or unstable fracture patterns (e.g., Barton's).
LaFontaine’s Criteria (Instability Risk): Dorsal comminution >50%, initial dorsal tilt >20°, intra-articular extension, associated ulna fracture, or age >60 years.
Methods:
Volar Locking Plates (VLP): The current "gold standard" for most DRFs.
External Fixation: Used for severely comminuted, open, or "bridging" cases (often combined with K-wires).
Distal Ulna Fixation: Only required if the DRUJ remains unstable after fixing the radius or if there is a significant ulnar head fracture.
7. Prognosis and Complications
Prognosis: Good to excellent in 80% of patients with anatomical restoration.
> Poor functional outcomes associated with
worker's compensation
low socioeconomic status
low education levels
low bone density
> Successful outcomes correlate with
accuracy of articular reduction
restoration of anatomic relationships
early efforts to regain motion of wrist and fingers
Complications:
Median Neuropathy: Acute carpal tunnel syndrome.( progressive paresthesias, weakness in thumb opposition, paresthesias that do not respond to reduction and last > 24-48 hours)
Ulnar Nerve Neuropathy:DRUJ injury
EPL Rupture (Extensor Pollicis Longus): Common in nondisplaced fractures due to localized ischemia at Lister's tubercle. Volar plating with screw fixation that penetrates the dorsal cortex and is proud dorsally
FPL Rupture: Very distal volar plate placement on the radius (distal to watershed line) is associated with FPL rupture
Malunion/Nonunion : Results in "radial shortening," causing ulnar impaction syndrome. intra-articular malunion (revision at > 6 weeks) , extra-articular angulation malunion (dorsal angulation > 10° from neutral results in increased stiffness of the interosseous membrane and limitation of simulated forearm pronation and supination) , radial shortening malunion (treatment-ulnar shortening)
CRPS (Complex Regional Pain Syndrome): Chronic pain and stiffness (Type 1). AAOS 2010 clinical practice guidelines recommend vitamin C supplementation to prevent incidence of RSD postoperatively, subsequent analyses show no benefit to vitamin C, strong evidence to suggest the efficacy of prompt physiotherapy, lidocaine, ketamine, bisphosphonates, sympathectomy and brachial plexus blocks.
DRUJ Instability: Persistent pain during supination/pronation.
Radiocarpal Arthrosis: (2-30%) 90% young adults will develop symptomatic arthrosis if articular stepoff > 1-2mm, may also be nonsymptomatic
ECU or EDM Entrapment: DRUJ injury
Compartment Syndrome
8. Key Points (Clinical Pearls)
Restore the Tilt: Restoring volar tilt and radial height is the primary goal to prevent long-term arthritis.
The Median Nerve is Priority: Immediate reduction is required if there are signs of median nerve compression.
Check the Ulna: Always re-evaluate the DRUJ after fixing the radius. If it is stable, ulnar styloid fractures usually don't need surgery.
Early Finger ROM: Start finger motion immediately to prevent tendon adhesion and CRPS.
References
Rockwood and Green’s Fractures in Adults: Detailed biomechanics and surgical approaches.
AO Principles of Fracture Management: The standard for AO/OTA classification and plating techniques.
Lafontaine M, et al.: Instability assessment of distal radius fractures. (Journal of Bone and Joint Surgery).
Rikli DA, Regazzoni P: The three column concept in distal radius fractures. (Journal of Hand Surgery).