1. General Overview & Epidemiology
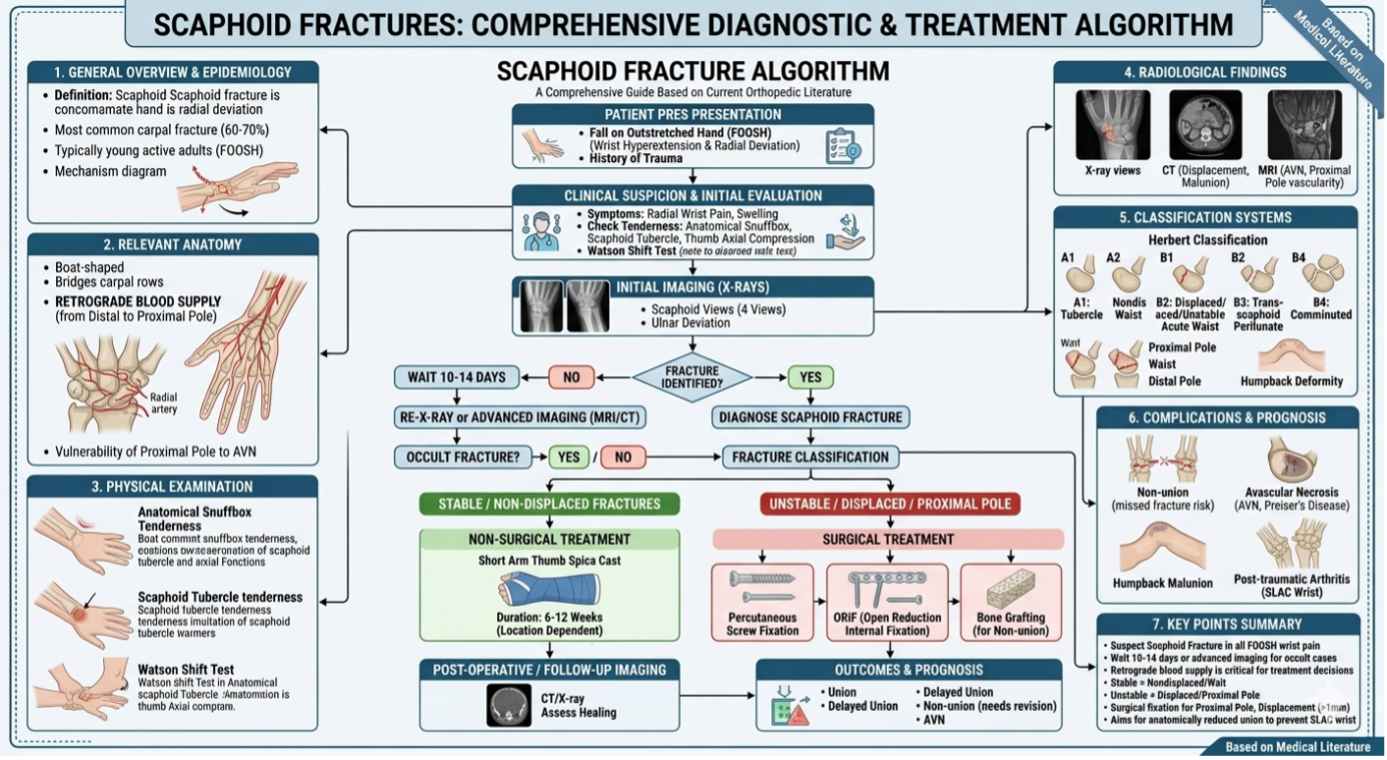
The scaphoid is the most commonly fractured carpal bone, accounting for approximately 60–70% of all carpal fractures and 11% of all hand fractures.
Demographics: Most prevalent in young, active males (2 :1 male : female) (ages 15–30). It is rare in children and the elderly, where the distal radius is more likely to break first.
Mechanism: Typically a fall on an outstretched hand (FOOSH) with the wrist in extension (>90°) and radial deviation.
2. Relevant Anatomy
The scaphoid's anatomy is its destiny. It is a boat-shaped bone that bridges the proximal and distal carpal rows. Complex 3-dimensional structure described as resembling a boat, skiff, and twisted peanut oriented obliquely from extremity's long-axis (implications for advanced imaging techniques) largest bone in proximal carpal row .
> 75% of scaphoid bone is covered by articular cartilage
articulates with radius, lunate, trapezium, trapezoid, and capitate
· Anatomic location
percentage of fractures by scaphoid anatomic location
waist -65%
proximal third - 25%
distal third - 10%
Historically the distal pole is most common location in pediatrics due to ossification sequence, however more recently waist fractures have become most common
Blood Supply: Crucially, the blood supply is retrograde. The branches of the radial artery enter the bone at the distal pole or waist and travel back to the proximal pole.
Vulnerability: Because of this retrograde flow, fractures at the "waist" or "proximal pole" often cut off the blood supply to the proximal fragment, leading to a high risk of Avascular Necrosis (AVN).
3. Clinical Presentation & Physical Examination
Clinical Complaints:
Dorsoradial wrist pain.
Weakness in grip and pinch.
The "sprained wrist" that doesn't get better.
Physical Examination Findings:
Anatomical Snuffbox Tenderness: High sensitivity (90%) but lower specificity.
Scaphoid Tubercle Tenderness: Palpated on the volar aspect of the wrist.
Thumb Axial Compression Test: Pain when pressure is applied along the long axis of the thumb.
Watson Shift Test: May be positive if associated ligamentous injury is present.
4. Radiological Findings
· Initial X-rays can be negative in up to 20 -30 % of cases. repeat radiographs in 14-21 days
Standard Series: PA, Lateral, Oblique (semi-pronated (45°)) , and the Scaphoid View (PA with 30° ulnar deviation and extension).
Bone scan: Occult fractures in acute setting . Specificity of 98%, and sensitivity of 100%, PPV 85% to 93% when done at 72 hours
MRI: The Gold Standard for diagnosing occult fractures (those not visible on X-ray) and assessing the vascularity of the proximal pole. approach 100% for occult fractures
CT Scan: Best for assessing fracture displacement, angulation (humpback deformity), and union status during follow-up.
5. Classification Systems
· The most widely used is the Herbert Classification, which focuses on stability:
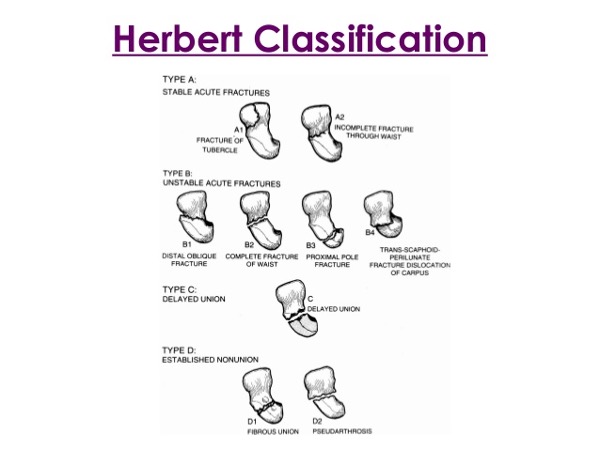
Type | Stability | Description & Examples |
Type A: Acute Stable | Stable | Small, incomplete, or non-displaced fractures. Examples: A1 (Tubercle), A2 (Non-displaced waist). |
Type B: Acute Unstable | Unstable | Fractures with a high risk of displacement or non-union. Examples: B1 (Distal oblique), B2 (Complete/displaced waist), B3 (Proximal pole), B4 (Trans-scaphoid perilunate). |
Type C: Delayed Union | Unstable | Fractures that have not healed within the expected timeframe (usually >6–12 weeks). Characterized by cyst formation and widening of the fracture line. |
Type D: Non-union | Established | Chronic failure of the bone to knit together. Can be "fibrous" (stable but not bone) or "pseudarthrosis" (unstable, forming a false joint). |
Mayo Mayo classification (based on location of fracture line)
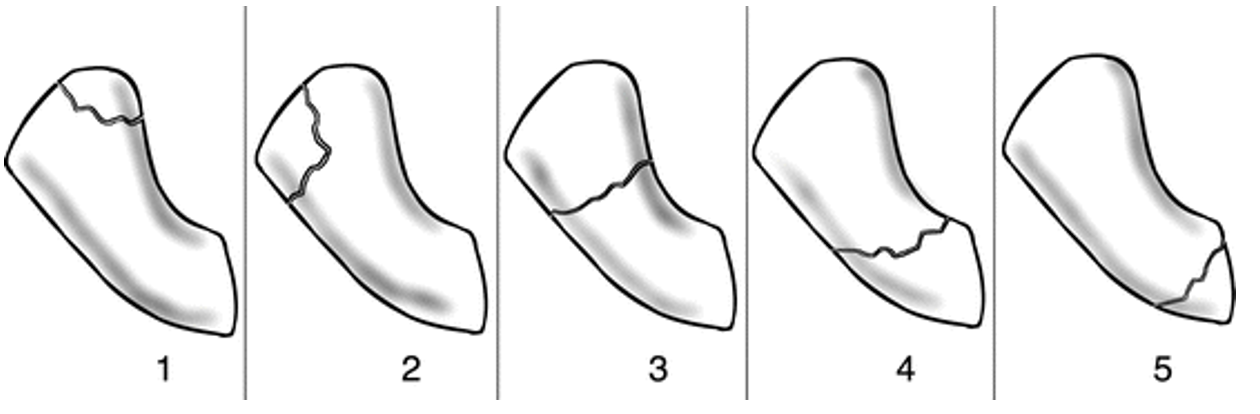
Type | Location | Clinical Significance |
Type I | Distal Tubercle | Extra-articular and generally stable; carries an excellent prognosis for healing with conservative treatment. |
Type II | Distal Articular Surface | Involves the joint surface; requires careful assessment for displacement to prevent secondary arthritis. |
Type III | Distal Third | Generally has a good blood supply and a high rate of union with cast immobilization. |
Type IV | Middle Third (Waist) | The most common fracture site (approx. 70–80%); considered the "watershed" area where stability and blood supply become more precarious. |
Type V | Proximal Third | High-risk area; often results in AVN or non-union because the fracture line frequently severs the retrograde blood supply to the proximal pole. |
Russe Classification (based on fracture pattern)
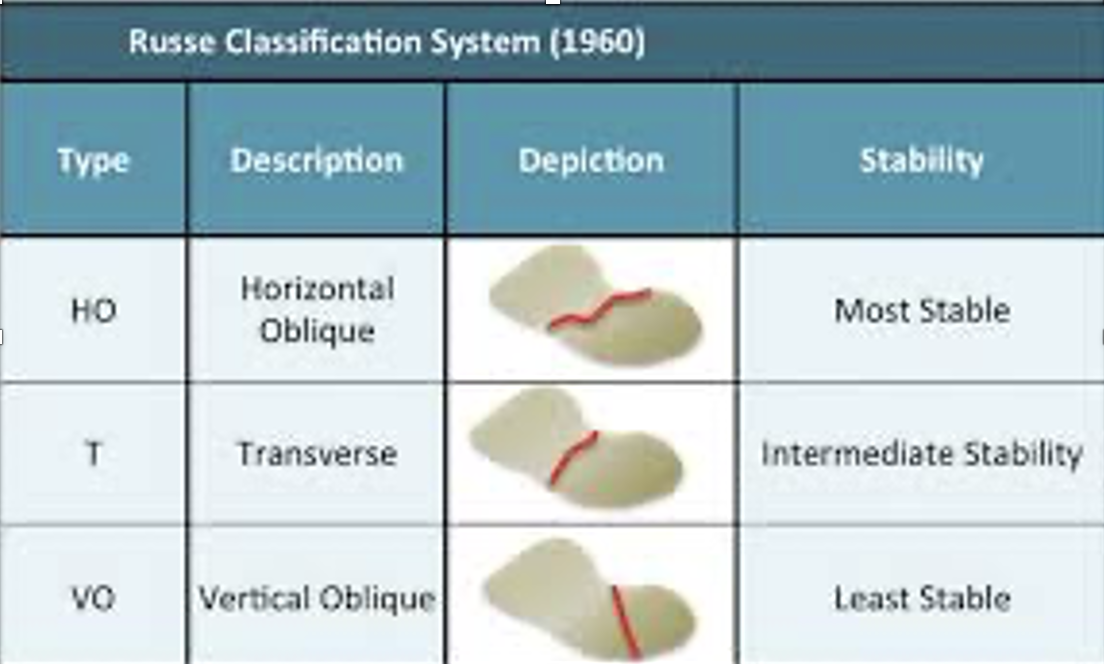
Type | Fracture Pattern | Stability Level | Biomechanical Effect |
Type I | Horizontal Oblique | Stable | The fracture line is perpendicular to the long axis; physiological loading creates compression, aiding union. |
Type II | Transverse | Intermediate | A straight horizontal line; generally stable but can displace if the "waist" is completely involved. |
Type III | Vertical Oblique | Highly Unstable | The fracture line is parallel to the long axis; loading creates shear/sliding forces that frequently lead to non-union. |
6. Treatment Strategies
Non-Surgical Treatment
Indications: Nondisplaced (distal pole or waist) stable fractures.
Management: Long-arm or short-arm Thumb Spica Cast. The inclusion of the thumb and the duration (typically 6–12 weeks) remain debated, but immobilization is key. scaphoid fractures with <1mm displacement have union rate of 90%
Surgical Treatment
Indications: Displaced fractures (>1mm), proximal pole fractures (due to AVN risk), unstable patterns, or athletes requiring early return to play.
Methods:
Percutaneous Screw Fixation: Minimally invasive using a headless compression screw (e.g., Herbert screw).
Open Reduction Internal Fixation (ORIF): Necessary for displaced fractures or those requiring bone grafting.
indications
significantly displaced fracture patterns
15° scaphoid humpback deformity
radiolunate angle > 15° (DISI)
intrascaphoid angle of > 35°
scaphoid fractures associated with perilunate dislocation
comminuted fractures
unstable vertical or oblique fractures
outcomes
accuracy of reduction correlated with rate of union
7. Prognosis and Complications
Prognosis: Good for distal fractures; becomes more guarded as the fracture moves proximally.
Complications:
· Non-union: Failure to heal, often leading to SLAC Wrist (Scaphoid Lunate Advanced Collapse). 5-10% following immobilization, higher rates for proximal pole fractures. Treatment isvascularized or nonvascularized bone grafting procedures
· Avascular Necrosis (AVN): Especially common in the proximal pole (Preiser’s disease). 13-50% of all scaphoid fractures
· Malunion: Often manifests as a "humpback deformity," which alters wrist biomechanics.
· Subchondral bone penetration with arthrosis due to prominent hardware
· SNAC wrist (scaphoid nonunion advanced collapse)
8. Key Points (Summary)
Suspect it in everyone: If there is snuffbox tenderness after a fall, treat it as a fracture until proven otherwise (the "suspected scaphoid" protocol).
Proximal = Problem: The more proximal the fracture, the higher the risk of AVN and non-union.
Vascularity is King: MRI is your best friend for evaluating the health of the bone.
Follow-up is mandatory: Do not dismiss a patient with a "normal" initial X-ray if clinical suspicion remains high.
Literature & References
Rockwood and Green's Fractures in Adults: Detailed section on carpal kinematics and retrograde blood supply.
Greene's Operative Hand Surgery: Comprehensive guide on surgical approaches and bone grafting techniques for non-union.
Herbert TJ, Fisher WE. Management of the fractured scaphoid using a new type of compression screw. J Bone Joint Surg Br. 1984.
Boyer MI, et al. Occult scaphoid fractures. J Hand Surg Am. 2002. (Discusses the role of early MRI).