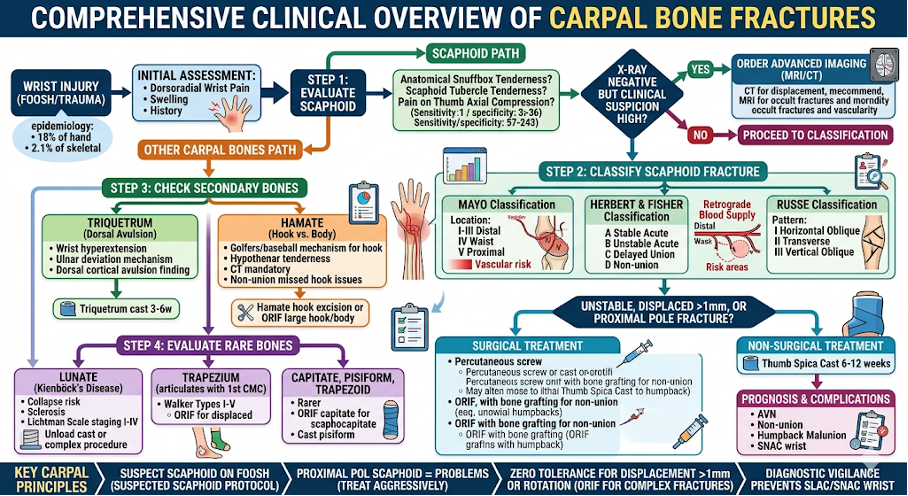
1. General Overview & Epidemiology
Frequency: The scaphoid is the most commonly fractured carpal bone, accounting for 60–70% of all carpal injuries.
Secondary Fractures: The triquetrum is the second most common (~14%), often occurring as a dorsal avulsion fracture. Treatment is generally nonoperative but injuries associated with wrist instability require surgical fixation. perilunate dislocations (seen in 12-25% of triquetral fractures)
Rare Injuries: Fractures of the lunate, capitate, hamate, trapezium (third most common carpal bone fracture) , trapezoid, and pisiform are relatively rare, each accounting for less than 5% of carpal injuries.
Demographics: These injuries predominantly affect young, active adults, often resulting from high-energy trauma or sports-related falls.
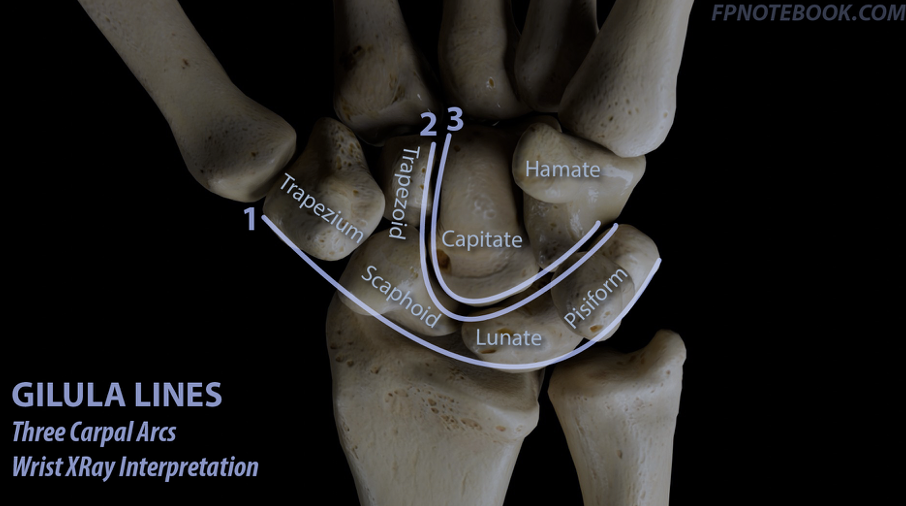
2. Relevant Anatomy
The carpus is organized into two functional rows that bridge the forearm to the metacarpals.
Proximal Row: Scaphoid, lunate, triquetrum, and pisiform.
Distal Row: Trapezium, trapezoid, capitate, and hamate.
Vascularity: The scaphoid is unique due to its retrograde blood supply. Blood enters distally and flows toward the proximal pole, making proximal fractures highly susceptible to avascular necrosis (AVN).
Articulations: The trapezium forms a specialized saddle joint with the first metacarpal, which is essential for thumb opposition and pinch power.
3. Clinical Presentation & Physical Examination
Common Complaints:
Acute dorsoradial wrist pain and swelling.
Weakness in grip and pinch power.
History of a Fall On An Outstretched Hand (FOOSH).
Physical Examination Findings:
Anatomical Snuffbox Tenderness: Highly sensitive for scaphoid fractures.
Scaphoid Tubercle Tenderness: Palpated on the volar aspect.
Thumb Axial Compression: Pain during long-axis pressure on the thumb.
Watson Shift Test: Used to assess for associated carpal instability or ligamentous injury.
Hook of Hamate Tenderness: Localized pain in the palm, often seen in athletes (golfers/baseball players).
4. Radiological Findings
Standard Series: AP, Lateral, Oblique, and dedicated Scaphoid Views (30° ulnar deviation). The triquetrum fractures = "pooping duck" sign represents dorsal cortical fractures
Trapezium Fractures :Bett View (optional views),Carpal Tunnel View (trapezial ridge fracture)
Hamate Body and Pisiform Fractures:ER Oblique View (best to see these fractures ) , Carpal Tunnel View
Roberts View: A hyper-pronated AP view used specifically to visualize the 1st CMC (Trapezium-Metacarpal) joint.
CT Scan: The gold standard for assessing fracture displacement (>1mm), comminution, and the orientation of the fracture line (Russe patterns).
MRI: Most sensitive for identifying occult fractures (not visible on initial X-ray) and evaluating the vascularity of the proximal pole.
5. Classification Systems
A. Scaphoid Fractures
Herbert and Fisher: Based on stability (Stable A1/A2, Unstable B1-B4, Delayed Union C, Non-union D).
Mayo: Based on anatomical location (Types I-V, from distal tubercle to proximal third).
Russe: Based on fracture line orientation (Horizontal Oblique, Transverse, Vertical Oblique) to predict shear forces.
B. Other Notable Classifications
Lunate: Often associated with Kienböck’s disease (avascular necrosis) or perilunate dislocations.
Triquetrum: Categorized as dorsal cortical avulsion fractures (common) or body fractures (rare/unstable).
Fracture Type | Prevalence & Mechanism | Subtypes & Clinical Notes |
Dorsal Cortical Fractures | Most common type, accounting for up to 93% of triquetrum injuries. Mechanisms include avulsion, shearing force, or impaction. | Typically results from wrist hyperextension and ulnar deviation. |
Body Fractures | Identified as the second most common pattern. Often requires advanced imaging (CT) for detailed evaluation. | Subtypes include sagittal, medial tuberosity, transverse proximal pole, transverse body, and comminuted patterns. |
Palmar Cortical Fractures | Mechanisms involve avulsion or shearing forces. | Carries a significant risk of instability, often associated with palmar ligamentous injury. |
Hamate: Categorized by fractures of the body vs. fractures of the hook.
Type | Location | Common Mechanism | Key Association |
I-I | Tip (Avulsion) | Ligamentous tension | Minimal symptoms |
I-II | Middle (Waist) | Sports (Golf/Baseball) | High non-union rate |
I-III | Base | Direct trauma | Ulnar nerve/FDP risk |
IIA | Body (Coronal) | Axial load/Punch | CMC Dislocation |
IIB | Body (Transverse) | Crush injury | Carpal instability |
Trapezium Fracture Classification
Category | Type / Classification | Mechanism & Clinical Characteristics |
Ridge Fractures | Type 1 | Involves the base of the ridge. |
Type 2 | Characterized by smaller avulsion fractures. | |
Body Fractures | Walker Classification | |
Vertical Intra-articular | Most common pattern; typically caused by axial compression. | |
Horizontal | Resulting from horizontal shear forces. | |
Dorsal Radial Tuberosity | Caused by vertical shear forces. | |
Anterior Medial Ridge | Involves loading or avulsion of the transverse carpal ligament. | |
Comminuted | High-energy injury resulting in multiple bone fragments. | |
Fracture-Dislocation | Result of high-energy injuries; frequently missed in clinical settings due to concomitant injuries. |
6. Treatment Strategies
Non-Surgical Treatment
Indications: Nondisplaced, stable fractures (e.g., Herbert Type A, Mayo I-III).
Method: Thumb Spica Cast or short-arm cast for 6–12 weeks depending on the bone and fracture location.
Surgical Treatment
Indications: Displaced fractures (>1mm), unstable patterns (Vertical Oblique/Russe III), proximal pole fractures, or intra-articular fractures involving the CMC joint (Bennett/Rolando patterns at the base of the thumb).
Methods:
§ Percutaneous Screw Fixation: Minimally invasive use of headless compression screws.
§ ORIF (Open Reduction Internal Fixation): Required for complex comminution (Rolando, Herbert B4) or fractures requiring bone grafting.
§ Pisiformectomy, Fragment excision, Trapeziectomy
§ Primary arthrodesis
§ External fixation
7. Prognosis and Complications
Prognosis: Generally excellent for distal fractures; becomes guarded for proximal fractures due to vascular risks.
Complications:
§ Avascular Necrosis (AVN): Highest risk in the proximal scaphoid and lunate.
§ Non-union: Often leads to SNAC (Scaphoid Non-union Advanced Collapse) or SLAC (Scaphoid Lunate Advanced Collapse) wrist arthritis.
§ Humpback Deformity: A malunion causing flexion of the scaphoid, altering wrist mechanics.
§ Ulnar nerve neuritis in Guyon's canal
§ Closed rupture of the flexor tendons to the small finger
§ Weakened grip strength
§ Recurrence after excision
8. Key Points (The "Gold Standard" Principles)
Zero Tolerance for Rotation: Even 1° of rotation can lead to significant functional overlap at the fingertips.
Suspect the Scaphoid: Any FOOSH with snuffbox tenderness should be treated as a fracture until MRI or follow-up X-rays prove otherwise.
Vascularity is King: Treatment decisions, especially in the scaphoid, are driven primarily by the risk of interrupting the retrograde blood supply.
Early Motion: Start range of motion (ROM) as soon as stability is achieved to prevent joint stiffness.
Literature & References
AO Principles of Fracture Management: Guidelines for internal fixation of carpal and metacarpal injuries.
Green’s Operative Hand Surgery: The definitive text for carpal anatomy and surgical approaches.
Herbert TJ, Fisher WE: Management of the fractured scaphoid using a new type of compression screw. JBJS Br, 1984.
Russe O: Fractures of the carpal navicular. JBJS, 1960.