Definition
Injury of the terminal extensor mechanism at the distal interphalangeal (DIP) joint, resulting in:
Inability to actively extend the DIP
Flexed resting position of the fingertip
Can be:
Tendinous (soft tissue)
Bony (avulsion fracture)
Epidemiology
Common finger injury
Seen in athletes and daily activities
Most often affects long and ring fingers
Mechanism of Injury
Sudden forced flexion of an extended DIP joint
Typical mechanism: ball striking fingertip
Pathophysiology
Terminal extensor tendon rupture
orAvulsion fracture of distal phalanx base
Clinical Presentation
Drooping fingertip
Pain and swelling at DIP
Loss of active extension
Physical Examination
Passive extension intact
Active extension absent
Imaging
X-ray mandatory
Evaluate:
Fracture size
Joint alignment
Subluxation
Classification
Wehbé–Schneider Classification
Type I
No volar subluxation
Type II
Volar subluxation of distal phalanx
Type III
Epiphyseal injury (pediatric)
Subtypes (Based on fracture size)
A: <1/3 articular surface
B: 1/3–2/3
C: >2/3
Clinical Interpretation
Type I → usually stable
Type II → unstable (surgical consideration)
Larger fragments → higher instability risk
Treatment
1.Nonoperative
Indications
Most Type I injuries
Stable bony mallet
Management
DIP splint in full extension
6–8 weeks continuous splinting
Followed by night splint

2.Operative Treatment
Indications
Volar subluxation (Type II)
Large fragment (>30–50%)
Failed conservative treatment
Open injury
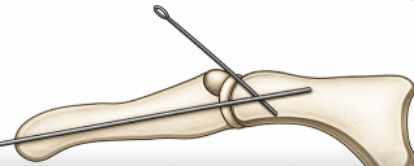
Techniques
Extension block pinning
Percutaneous pinning
ORIF (rare)
Complications
Extension lag
Swan neck deformity
Skin problems from splint
Joint stiffness
Prognosis
Generally excellent
Mild extension lag common but well tolerated
Pits & Pearls
Splint compliance = most important factor
Even brief DIP flexion resets healing
Most cases treated conservatively
Classification helps identify unstable injuries
Pitfalls
Missing subluxation on X-ray
Poor splinting technique
Early discontinuation of splint
Underestimating large fragments