· Overview
- Extensor tendons are dorsally located, thin, and flat, making them relatively weak against tensile forces and prone to adhesion formation.
- Compared to flexor tendons:
o They have less tendon excursion
o Their broader surface area increases the risk of adhesions
o They have lower capacity to hold core sutures
- Common mechanisms of injury include:
o Sharp lacerations (most common)
o Crush or avulsion injuries
o “Fight bite” injuries (particularly important in zone 5)
· Anatomy
Tendons
- EDC (Extensor Digitorum Communis): Primary extensor
- EIP (Extensor Indicis Proprius): Independent extension of the index finger
- EDM (Extensor Digiti Minimi): Extension of the small finger
- EPL/EPB (Extensor Pollicis Longus / Brevis): Thumb extension
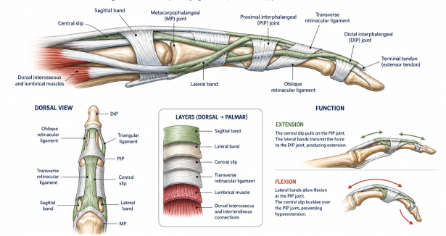
Extensor Mechanism
- Central slip -> Extension of the PIP joint
- Lateral bands -> Extension of the DIP joint
- Sagittal bands -> Stabilization of the MP joint
- Triangular ligament -> Stabilization of the lateral bands
- ORL (oblique retinacular ligament):
> Synchronizes motion between the PIP and DIP joints
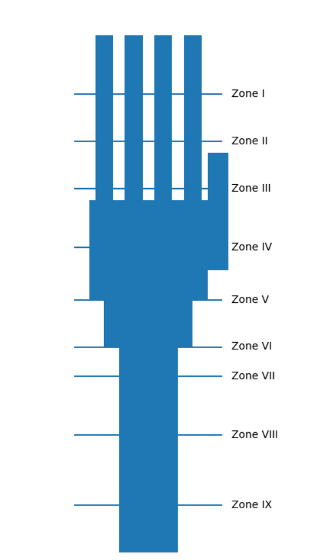
· Zones of Injury
Zone | Location | Clinical Significance |
1 | DIP joint | Mallet finger |
2 | Middle phalanx | Rare |
3 | PIP joint | Boutonnière deformity |
4 | Proximal phalanx | Tendon becomes thicker |
5 | MP joint | ‘’Fight bite’’ injuries |
6 | Metacarpal | Favorable prognosis |
7 | Wrist | Under the extensor retinaculum |
8 | Distal forearm | Musculotendinous junction (MTJ) |
9 | Proximal forearm | Muscle belly involvement |
· Clinical Evaluation
o Loss of active extension
o Assessment of the tenodesis effect
o In open injuries:
§ The tendon may not be visible -> maintain a high index of suspicion
o Zone 5 injuries:
§ High risk of infection (due to oral flora)
· Imaging
o X-ray
§ Fractures
§ Foreign bodies
o USG
§ Partial tendon lacerations
o MRI, rarely indicated
· Treatment Principles
o Genel yaklaşım
§ <%50 tendon kesisi -> konservatif
§ %50 -> cerrahi onarım
· Zone – based Treatment
o Zone 1
§ Terminal extensor tendon rupture (mallet finger)
§ Loss of DIP extension, flexion deformity
§ Nonoperative treatment:
· DIP extension splint x 6-8 weeks (full time)
§ Operative indications:
· Large avulsion fragment
· Volar subluxation
· Open injury
§ Pearl:
· Any flexion during splinting -> treatment failure
o Zone 2
§ Usually treated conservatively
§ Large defects -> primary repair
o Zone 3 (central slip)
§ PIP ekstansiyon splinti (6 hafta)
§ Açık yaralanma -> cerrahi
o Zone 4
§ Core suture repair (4-0 / 5-0)
§ Dynamic splinting is recommended
o Zone 5 (MP joint)
§ Often open injuries
§ Debridement + antibiotics
§ Primary repair
o Zone 6
§ Best outcomes
§ Core sutures are easier to apply
§ RMS (relative motion splint) is highly effective
o Zone 7
§ Preserve the extensor retinaculum
§ Tendon retraction may occur
§ Tendon transfer may be required
o Zone 8-9
§ Muscle belly involvement
§ Weak repair strength
§ Tendon grafting or transfer may be necessary
· Rehabilitation
o Early controlled motion (to prevent adhesions)
o Dynamic splinting:
§ Extension - assisted
o RMS (Relative Motion Splint):
§ Positions the MP joint in relative extension
· Complications
o Adhesions (most common)
o Extensor lag
o Tendon rupture
o Joint stiffness