OVERVIEW
· Flexor tendon injuries are among the most critical emergencies in hand surgery.
· Goal: restore tendon continuity + preserve smooth gliding
· Most challenging area: Zone 2 (“no man’s land”)
· Treatment success depends on the combination of surgical technique and rehabilitation
Anatomy
· Two main tendons:
o FDS (flexor digitorum superficialis) -> PIP flexion
o FDP (flexor digitorum profundus) -> DIP flexion
· Camper’s chiasma
o FDS splits into two slips, allowing FDP to pass through
· Pulley system
o Critical pulleys: A2 and A4 (must be preserved!)
o Function: prevents tendon bowstringing.
· Blood supply
o Vincula system (VBS, VBP)
o Zone 2 is relatively hypovascular
Classification
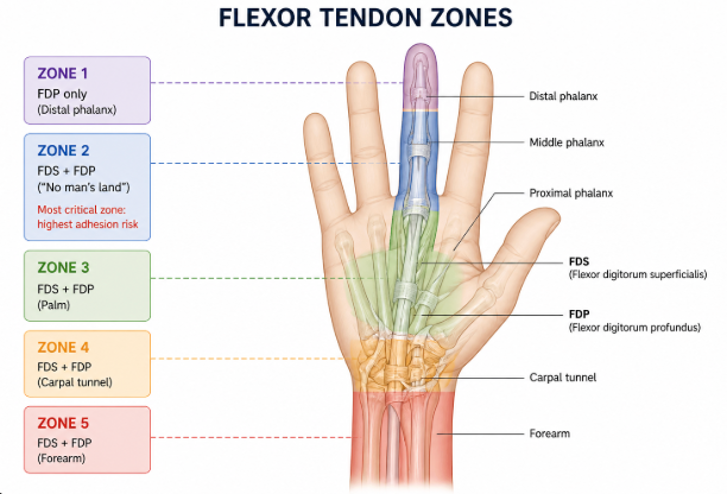
· Flexor tendon zones
o Zone 1: FDP distal, no FDS
o Zone 2: FDS + FDP (critical zone)
o Zone 3: palm
o Zone 4: carpal tunnel
o Zone 5: forearm
Most important: Zone 2 -> most difficult surgery + highest adhesion risk
Etiology
· Sharp lacerations (most common)
· Crush/avulsion injuries (jersey finger)
· İatrogenic
Clinical Presentation
· Loss of active flexion
· Pain
· History of open injury
· FDP injury -> loss of DIP flexion
· FDS injury -> loss of PIP flexion
Physical Examination
· FDS test
o Other fingers held in extension → assess PIP flexion
· FDP test
o PIP stabilized → assess DIP flexion
· Loss of tenodesis effect
· Painful flexion in partial injuries
Neurovascular Exam
· Two-point discrimination
· Capillary refill
· Evaluation for digital artery injury
Imaging
· Usually not required
· In suspicious cases:
o Ultrasound
o MRI
Treatment Principles
· Goals:
o Restore tendon continuity
o Maintain smooth gliding surface
o Enable early mobilization
Nonoperative Management
· Indications:
o <%50 partial lacerations
· Treatment:
o Splinting
o Early controlled mobilization
Operative Management
· Indications:
o Complete lacerations
o >%50 partial lacerations
o Functional deficit
Surgical Techniques
· Core suture
o Most important factor: suture strength
o Preferred:
4-strand or 6- strand repair
o Techniques:
Modified Kessler
Strickland
Cruciate
· Epitendinous suture
o Increases repair strength
o Improves tendon gliding
· Technical Principles
o Minimal tissue trauma
o Precise tendon end approximation
o Preserve pulleys (especially A2–A4)
o Pulley venting may be performed if necessary
· Zone Specific Management
Zone 1 Injury (FDP Avulsion)
· <1 cm stump -> tendon-to-bone repair
· >1 cm -> advancement possible
o Pull-out suture
o Suture anchor
Zone 2 Injury (Most Critical)
· Incolves both FDS and FDP
· High risk of adhesions
o Treatment:
ð Primary repair
ð Multistrand core + epitendinous repair
o Note:
ð One slip of FDS may be excised if necessary
Postoperative Care
· Dorsal splint:
o Wrist in flexion
o MCP joints in flexion
o IP joints in slight flexion
· Early controlled mobilization (very important)
o Duran/Kleinert protocols
Complications
· Adhesions (most common)
· Tendon rupture
· Quadriga effect
· Bowstringing
· Joint contracture
Prognosis
· Best outcomes:
o Early repair (<1 week)
o Effective rehabilitation
· Poor prognosis:
o Zone 2 injuries
o Crush injuries
o Delayed surgery
Pearls
· Use multistrand repair
· Do not forget epitendinous sutures
· Check tendon gliding intraoperatively
Pitfalls
· Excessive tension → rupture
· Pulley damage → bowstringing
· Poor rehabilitation → adhesions