Figures
1. General Overview & Epidemiology
Phalanx fractures account for approximately 10% of all human fractures. The distal phalanx is the most frequently injured bone in the hand, often due to crush injuries.
Demographics: Highest incidence occurs in males aged 15–35 (sports and machinery injuries) and elderly females (falls). more common in males 2:1
Mechanism: Direct impact (crush), indirect forces (torsion/rotational), or avulsion forces (tendon pulls).
Location
distal phalanx > middle phalanx > proximal phalanx
small finger is most commonly affected ( 38% of all hand fractures)
2. Relevant Anatomy
The hand consists of 14 phalanges. Understanding the tendinous attachments is critical for predicting fracture displacement:
Proximial Phalanx (PPx): No tendon insertions on the shaft. The interossei flex the proximal fragment, while the extensor mechanism pulls the distal fragment into extension, typically causing apex-volar angulation.
Middle Phalanx (MPx):
Fractures proximal to the flexor digitorum superficialis (FDS) insertion result in apex-dorsal angulation.
Fractures distal to the FDS insertion result in apex-volar angulation.
Distal Phalanx (DPx): Primarily stabilized by the fibrous septa of the pulp and the nail bed.
3. Clinical Presentation & Physical Examination
PRİMARİLY
· hand dominance
· baseline function
· occupation and hobbies
· mechanism of injury
Clinical Complaints:
Acute pain, swelling, and localized tenderness.
Deformity or "shortening" of the finger.
Inability to perform a full fist.
Physical Examination Findings:
Rotational Deformity: Crucial to check. With the fingers partially flexed, all fingernails should face the same plane, and the tips should point toward the scaphoid tubercle.
Digital Nerve/Vessel Status: Assess capillary refill and two-point discrimination.
Soft Tissue Integrity: Check for open fractures or nail bed lacerations (indicating an open fracture of the DPx).
4. Radiological Findings
Standard imaging includes Posteroanterior (PA), Lateral, and Oblique views.
Lateral View: Essential for determining the degree of angulation and joint involvement.
Stress Views: May be used if ligamentous avulsion (e.g., Gamekeeper’s thumb) is suspected but stable on static films.
CT scan
indications
assess articular involvement
findings
amount of articular displacement
degree of comminution
Differential Diagnosis
Stress fracture
Jammed finger
fracture-dislocation
gout
finger infection
neoplasm
5. Classification Systems
While many fractures are described descriptively (transverse, spiral, comminuted), specific systems include:
Location: Extra-articular vs. Intra-articular (base, shaft, or condylar).
Stability: Stable (undisplaced) vs. Unstable.
London Classification: Often used for subungual hematomas and distal phalanx fractures.
open vs closed
Proximal phalanx
location
head fractures
type I - stable with no displacement
type II - unstable unicondylar
type III - unstable bicondylar or comminuted
neck/shaft fractures
short oblique
long oblique
spiral
transverse
base fractures
extra-articular
intra-articular
lateral base
Middle phalanx
location
head fractures
type I - stable with no displacement
type II - unstable unicondylar
type III - unstable bicondylar or comminuted
neck fractures
apex volar angulation
shaft fractures
transverse
short oblique
long oblique
spiral
deformity
apex volar angulation
distal to FDS insertion
apex dorsal angulation
proximal to FDS insertion
without angulation
due to inherent stability provided by an intact and prolonged FDS insertion
base fractures
deformity is usually apex dorsal angulation
proximal fragment in extension (due to central slip)
distal fragment in flexion (due to FDS)
can be further classified into
partial articular fractures
volar base
results from hyperextension injury or axial loading
represents avulsion of volar plate
unstable if > 40% articular surface involved
dorsal base
results from hyperflexion injury
represents avulsion of central tendon
lateral base
represents avulsion of collateral ligaments
complete articular fractures
know as pilon fractures
unstable in all directions
Distal phalanx
tuft fractures
mechanism is usually crush injury
usually stable due to nail plate dorsally and pulp volarly
often associated with laceration of nail matrix or pulp
shaft fractures
can be
transverse
longitudinal
base fractures
usually unstable
mechanism can be
shearing due to axial load, leading to fracture involving > 20% of articular surface
avulsion due tensile force of terminal tendon or FDP, leading to small avulsion fracture
can be further classified into
volar base
dorsal base
SEYMOUR FRACTURES
epiphyseal injury of distal phalanx
resuls from hyperflexion
presents as mallet deformity (i.e. apex dorsal) due to
terminal tendon attaches to proximal epiphyseal fragment
FDP attaches to distal fragment
intra-articular vs extra-articular
fracture morphology
amount of displacement
open vs closed
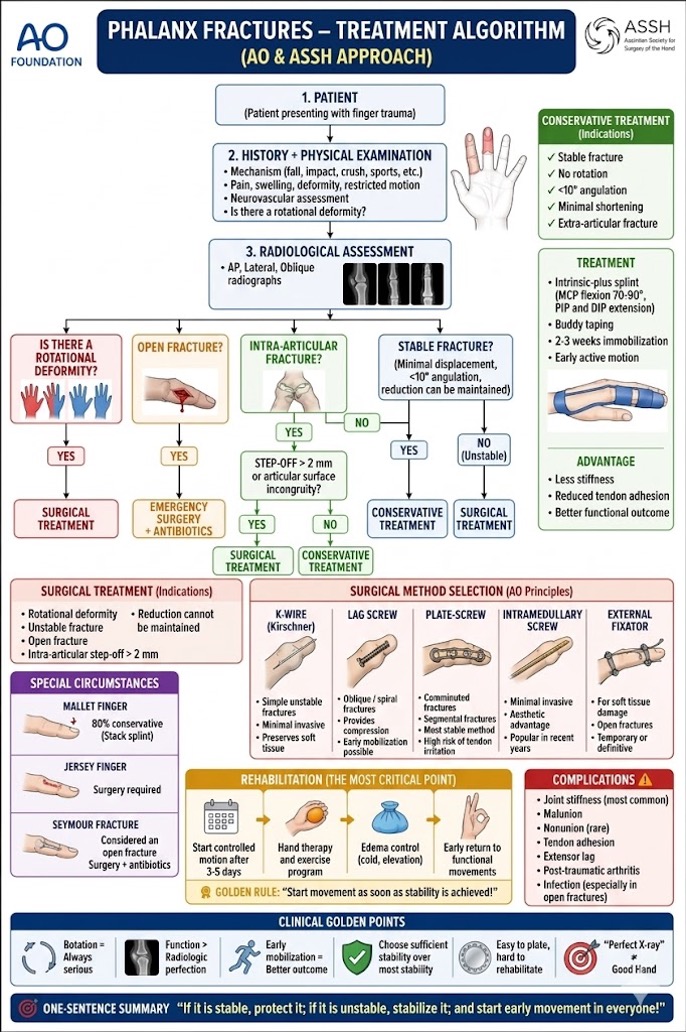
6. Treatment Strategies
Non-Surgical Treatment
Indicated for stable, non-displaced, or reducible fractures.
Buddy Taping: For stable fractures; allows early range of motion (ROM).
Splinting: Typically the MCP joint is held in 60–70° flexion (intrinsic plus position) to prevent collateral ligament shortening.
Duration: Usually 3–4 weeks, followed by aggressive mobilization.
Surgical Treatment
Indicated for unstable, open, or irreducible fractures, and those with significant rotational deformity.
Percutaneous K-wire Fixation: Versatile and minimally invasive but requires pin care.
ORIF (Open Reduction Internal Fixation): Uses mini-plates and screws. Provides rigid fixation allowing for immediate ROM.
Intramedullary Heading: Used for certain transverse shaft fractures.
7. Prognosis and Complications
Prognosis: Generally excellent with timely treatment, though some loss of terminal flexion is common.
Complications:
Stiffness (Tendon Adhesions): The most common complication. Treatment with aggressive hand therapyfirst-line treatmentsurgical release failed nonoperative treatment
· Malunion: Resulting in "scissoring" of fingers during flexion. treatment
Nonoperative (asymptomatic, no functional impairment )
Surgery (indicated when associated with functional impairment
options
corrective osteotomy at malunion site (preferred)
metacarpal osteotomy (limited degree of correction)
· Non-union: Rare in the phalanges due to high vascularity. (<2%) most atrophic and associated with bone loss or neurovascular compromise
surgical options
resection, bone grafting, plating
ray amputation or fusion
Post-traumatic Arthritis: Common in poorly reduced intra-articular fractures.
8. Key Points (Summary)
Check Rotation: Clinical rotation is more important than radiographic appearance.
Early Motion: "Movement is life" for hand fractures to prevent adhesion.
Apex-Volar: The most common angulation for proximal phalanx fractures.
Nail Bed: Always treat nail bed lacerations associated with DPx fractures as open fractures.
Literature & References
Rockwood and Green's Fractures in Adults: The gold standard for hand fracture biomechanics and fixation.
Greene's Operative Hand Surgery: Detailed surgical techniques and outcomes.
Journal of Hand Surgery (JHS): Recent studies emphasize the shift toward "wide-awake local anesthesia no tourniquet" (WALANT) for intraoperative assessment of stability.
Belsky MR, et al.: Classic studies on the conservative management of extra-articular fractures.
AO Foundation - Phalangeal fracture treatment algorithm