Summary[1]
Rare but severe traumatic injuries.
Commonly associated with high-energy trauma; high risk of neurovascular complications.
Historically, prognosis has been variable and treatment approaches controversial.
Current evidence confirms that early management strongly influences long-term outcomes.
Typically involve multiligamentous injuries with vascular and neurological complications.
Clinical suspicion is critical; vascular protocols must be applied, and neurovascular exam repeated after reduction.
Epidemiology[2]
Account for about 0.02% of all orthopaedic injuries.
More frequent in obese patients due to low-energy mechanisms.
High-energy trauma (e.g., motor vehicle accidents) is the most common cause, but low-energy sports-related injuries are also observed.
Pathophysiology and Anatomy[2,3]
Bones/joints: Femur, tibia, patella, tibiofemoral joint, patellofemoral joint.
Ligaments: ACL, PCL, MCL, LCL.
Menisci: Medial and lateral.
Muscles: Quadriceps, iliotibial band, biceps femoris, popliteus, pes anserinus group, semimembranosus, gastrocnemius, plantaris.
Nerves: Tibial, femoral, sciatic, peroneal branches; posterior/lateral femoral cutaneous, sural, saphenous, obturator.
Mechanism of Injury[4]
High-energy: Motor vehicle accidents; cause extensive soft tissue and neurovascular damage.
Low-energy: Sports injuries; lower complication rates but still clinically significant.
Anterior dislocation: Forced hyperextension (traffic accidents, football, rugby, stepping into a hole).
Posterior dislocation: Posterior force applied to tibia with knee flexed (dashboard injury, fall onto flexed knee).
Less common: Direct blows or missteps.
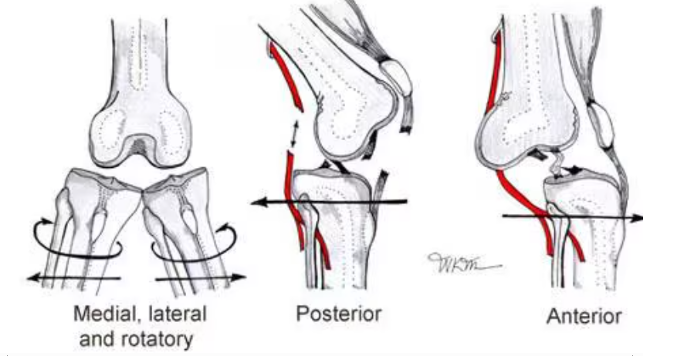
Figure 1:Types of knee dislocation.(Cited from www.emedicine.medscape.com)
Classification:[5]
Acute: < 3 weeks post injury
Chronic: > 3 weeks post injury
Kennedy Classification [5]
Direction | Mechanism | Injury Pattern |
Anterior | Hyperextension | Posterior capsule,PCL,ACL injury |
Posterior | Dashboard | PCL injury |
Medial | Varus/rotation | Collaterals,crucirate |
Lateral | Valgus, flexion/adduction | Collaterals,crucirate |
Rotatory | Rotation around PLC | MCL,ACL,PCL injury |
Schenck Classification[15]
KD I: Multiligamentous injury with involvement of either the ACL or PCL.
KD II: Injury to 2 ligaments: the ACL and PCL only.
KD III: Injury to 3 ligaments: the ACL and PCL, in addition to either the PMC or PLC.
KD IIIM: Involves the ACL, PCL, and MCL
KD IIIL: Involves the ACL, PCL, and LCL.
KD IV: Injury to 4 ligaments, including the ACL, PCL, PMC, and PLC. KD IV injuries have the highest rate of concomitant vascular injury (5% to 15%).
KD V: A multiligamentous injury with a periarticular fracture
Symptoms and Physical Examination [6,7,8,9,10]
History: Trauma with pain, deformity, and instability.
Priority: Assessment of life-threatening injuries in polytrauma patients.
Local exam: Deformity, open wounds, range of motion, extensor mechanism integrity.
Special tests:
ACL → Lachman
PCL → Posterior drawer
MCL/LCL → Varus/valgus stress tests
PLC → Dial test
Neurovascular exam (most critical):
Delay → Compartment syndrome or amputation (>85% if warm ischemia >6 hours).
Check dorsalis pedis and posterior tibial pulses; asymmetry/hematoma highly suspicious for vascular injury.
Imaging[11,12,13,14]
X-ray: First-line to detect fractures and malalignment.
Post-reduction X-ray: Confirms alignment, excludes irreducible PCL or avulsions.
Stress radiographs: Evaluate collateral/cruciate stability.
MRI: Best for multiligamentous and soft tissue injuries; guides diagnosis and treatment.
Examination under anaesthesia: Provides most accurate functional assessment by eliminating protective reflexes and pain.

Figure 2: X-ray knee dislocation (Cited from www.ce.mayo.edu/orthopedic-surgery/content/knee-dislocation-and-multiple-ligament-reconstruction-2017)
Complications [15,16,17]
Arthrofibrosis (most common): Associated with delayed mobilisation.
Laxity/instability: May persist; redislocation is rare.
Peroneal nerve injury: Frequent; about half recover spontaneously, others may need repair or tendon transfer.
Vascular injury (most severe): Directly linked with limb loss.
Treatment [18,19,20,21]
Nonoperative: Urgent closed reduction + neurovascular exam; vascular repair can follow if needed.
Open reduction: For irreducible, open, or posterolateral dislocations, or when vascular injury is present.
External fixation: Used in polytrauma, open fracture-dislocation, compartment syndrome, or after vascular repair.
Vascular repair: Emergent surgery with prophylactic fasciotomy.
Ligament reconstruction/repair: For persistent instability; early mobilisation is essential.
Nerve injuries:
Acute: Ankle-foot orthosis (AFO).
Persistent: Neurolysis, repair, or tendon transfer.