Introduction
The medial collateral ligament (MCL) is the primary static stabilizer of the knee against valgus stress and contributes significantly to rotational control. It is the most commonly injured ligament in the knee, either in isolation or in association with cruciate ligament injuries. Historically, nonoperative treatment has been the standard; however, current evidence indicates that surgical intervention is warranted in specific cases such as chronic instability or combined ligament injuries.
Anatomy and Biomechanics
The MCL complex comprises superficial (sMCL) and deep (dMCL) layers.
The sMCL originates from the medial femoral epicondyle and inserts distally into the tibia, providing resistance to valgus and external rotational forces.
The dMCL is a thickening of the medial capsule and connects to the medial meniscus, contributing to joint congruence and medial stability.
The posteromedial corner (PMC), including the posterior oblique ligament (POL), acts synergistically with the MCL to resist anteromedial rotatory instability.
Clinical Assessment
Patients typically report medial knee pain and swelling following valgus or twisting trauma. On physical examination, valgus stress testing at 30° flexion isolates the MCL, while laxity in full extension suggests additional cruciate or PMC involvement. A thorough assessment of ACL, PCL, and PMC function is mandatory.
Imaging and Classification
The American Medical Association (AMA) classifies MCL injuries into Grades I–III based on laxity and integrity:
Grade I: Mild sprain without instability
Grade II: Partial tear with moderate laxity
Grade III: Complete rupture
Standard imaging includes anteroposterior (AP) and lateral radiographs, with stress views optionally performed in skeletally immature patients to assess for widening or separation from a physeal fracture. MRI remains the gold standard for localizing the lesion, assessing severity, and identifying combined injuries.(Figure-1)
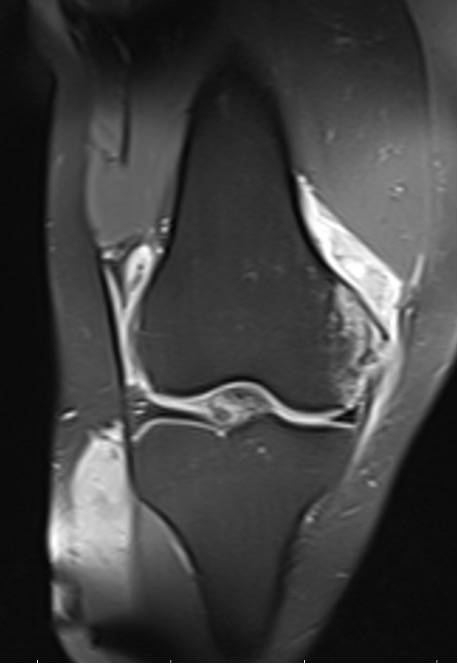
Figure-1 T2 weighted coronal MRI image showing ruptured of superficial MCL from 1/3 proximal portion
Figure Reference
Personal archive
Treatment Approaches
Nonoperative management remains effective for most isolated injuries. Early use of hinged knee bracing, controlled range-of-motion (ROM), and progressive strengthening exercises are fundamental.
Surgical treatment is indicated for:
Stener-like lesions (interposition of soft tissue)
Chronic symptomatic instability
Multiligament knee injuries (MLKI)
Acute tears may be repaired directly, while chronic or failed cases require anatomic reconstruction using autograft or allograft. Techniques such as LaPrade’s anatomic double-bundle and Xu’s triangular vector reconstruction are commonly used, with internal bracing facilitating earlier rehabilitation.
Postoperative Rehabilitation and Prognosis
Rehabilitation emphasizes early controlled motion to prevent stiffness, followed by quadriceps and hamstring strengthening. Internal bracing allows accelerated recovery protocols. Most patients regain near-normal stability and function if managed appropriately.
Conclusion
For orthopedic practice, understanding the anatomy, injury mechanism, and tailored management of MCL injuries is essential. While conservative therapy remains the cornerstone, surgical reconstruction provides excellent outcomes in complex or chronic cases, ensuring optimal knee stability and function.
References
* Vosoughi F, Rezaei Dogahe R, Nuri A, Ayati Firoozabadi M, Mortazavi J. Medial Collateral Ligament Injury of the Knee: A Review on Current Concept and Management. Arch Bone Jt Surg. 2021;9(3):255-262. doi:10.22038/abjs.2021.48458.2401
* Wijdicks CA, Griffith CJ, Johansen S, Engebretsen L, LaPrade RF. Injuries to the medial collateral ligament and associated medial structures of the knee. J Bone Joint Surg Am. 2010;92(5):1266-1280. doi:10.2106/JBJS.I.01229
* Pandey V, Khanna V, Madi S, Tripathi A, Acharya K. Clinical outcome of primary medial collateral ligament-posteromedial corner repair with or without staged anterior cruciate ligament reconstruction. Injury. 2017;48(6):1236-1242. doi:10.1016/j.injury.2017.03.021