Overview
23-42 persons/100,000 per-year first-time (primary) patellar dislocation
Often young skeletally immature adolescents, higher incidence among female patients.
17%- 66% treated nonsurgically experience further dislocations.
Patellofemoral instability - significant pain, increased risk of cartilage deterioration, reduced quality of life, lack of confidence at the knee and significant financial cost
Clinical Presentation
Objective patellar instability: at least one reported episode of lateral patellar dislocation with an identified anatomical risk factor.
Potential patellar instability (PPI/PPD): defined by the existence of anatomical risk factors associated with knee discomfort, although lacking of any documented cases of complete patellar dislocation.
Painful patellar syndrome (PPS): individuals in this classification show knee pain without specific anatomical risk factors or documented subluxation/dislocation episodes.
Clinical presentation - significant pain, lack of confidence at the knee with the fear of patellar dislocation
Risk factors:
Anatomical- Trochlea dysplasia, Patella alta, coronal and torsional (frontal) malalignment, lateral position of tibial tubercule
Others: age, hyperlaxity, trauma intensity
Physical examination: Apprehension test, patellar tilt test, J sign
Imaging
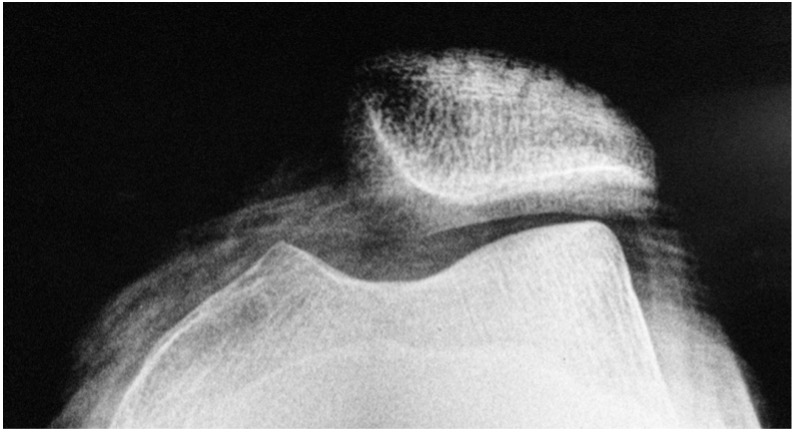
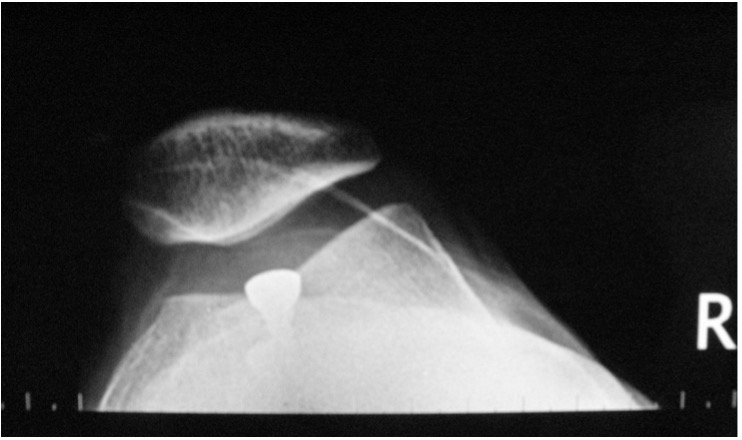
Lateral knee radiograps:
Trochlear dysplasia- supratrochlear spur, crossing sign and double contour
Patella alta: Caton-Deschamps index
Computerised Tomography: CT improved the classification of trochlear dysplasia and is used for the measurement TT-TG distance.
Magnetic resonance(MR): MR imaging is used for detection of cartilage lesions, soft tissue pathologies, measurement of patellotrochlear index and TT-TG distance.
Treatment
The Lyon School of Knee Surgery first developed the "menu a la carte" method in 1987, and it has since guided the treatment of patellar instability by treating each patient's most relevant anatomical risk factors one at a time.
Nonoperative treatment
First time patellar dislocation without loose bodies, osteochondral injury or associated injuries requiring surgery can be managed non-operatively.
Operative treatment
MPFL reconstruction
The MPFL functions as the primary biomechanical restraint preventing lateral dislocation during early flexion.
The reconstruction of MPFL is primary rule in the treatment strategy in any patient presenting patellofemoral instability following a prior dislocation.
Isolated MPFLR is most appropriate - exhibiting grade 1 trochlear dysplasia, in the absence of patella alta or an increased tibial tuberosity–trochlear groove (TT–TG) distance.
MPFL reconstruction can be added systematically in addition to the other procedures such as tibial tubercle osteotomy, trochleoplasty, vs at the end of the procedures.
Lateral release
The lateral release or lengthening- always combined with other procedures. It is indicated for patients with a negative medial tilt.
Lower limb osteotomies
>35 degrees of excessive femoral anteversion and >40 degrees of external tibial torsion are the thresholds for the derotational osteotomies for patellar instability.
Tibial tubercle osteotomy
Medialisation, anteriorisation and distalisation can be combined at the same procedure. Different threshold values are available in the literature with TT-TG distance of 15-20 mm. Functional patella alta(CDI>1.16 and sagittal patellofemoral engagement<%38) is indication for distalisation of tibial tubercle.
Trochleoplasty
Trochleoplasty is a surgical procedure that corrects the form and position of the trochlear groove to enhance the congruence of the articulating surfaces and prevent repeated patellar dislocations.
There are three surgical techniques. the lateral wedge augmentation trochleoplasty (LWAT), the recession trochleoplasty (RT) and the deepening trochleoplasty(DT).
The surgical for trochleoplasty is Dejour type 3 trochlear dysplasia(sulcus angle >157 or unmeasurable, LTI <14° or unmeasurable and central bump >5 mm.).
Differential Diagnosis
Anterior cruciate ligament injury- confused with especially first time patellar dislocation, lack of confidence at the knee in rotational stability.
Anterior knee pain
References
Atkin DM, Fithian DC, Marangi KS, Stone ML, Dobson BE, Mendelsohn C. Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury. Am J Sports Med. 2000;28(4):472-479.
Dejour H, Walch G, Nove-Josserand L, et al. Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc 1994 2 19–26. (https://doi.org/10.1007/bf01552649)
Dejour, D. H., Mazy, D., Pineda, T., Cance, N., Dan, M. J., & Giovannetti de Sanctis, E. (2025). Patellar instability: current approach. EFORT Open Reviews, 10(6), 378-387. Retrieved Aug 29, 2025, from https://doi.org/10.1530/EOR-2025-0051
El Attal, R., Kaiser, P. (2020). Derotational Osteotomies in Patella Instability. In: Dejour, D., Zaffagnini, S., Arendt, E., Sillanpää, P., Dirisamer, F. (eds) Patellofemoral Pain, Instability, and Arthritis. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-61097-8_51
Hinckel B, Smith J, Tanaka MJ, Matsushita T, Martinez-Cano JP. Patellofemoral instability part 1 (When to operate and soft tissue procedures): State of the art. J ISAKOS. 2025 Feb;10:100278. doi: 10.1016/j.jisako.2024.05.013. Epub 2024 May 23. PMID: 38795864.
Hinckel BB, Liebensteiner M, Smith JT, Gomes Gobbi R, Arendt EA. Patellofemoral instability part 2 (Bony procedure for patellar surgical stabilization): State of the art. J ISAKOS. 2025 Feb;10:100347. doi: 10.1016/j.jisako.2024.100347. Epub 2024 Oct 21. PMID: 39442805.