1. Overview
Posterolateral corner (PLC) injuries represent up to 16% of knee ligament injuries. They often occur with cruciate ligament injuries, especially the posterior cruciate ligament (PCL). Isolated PLC injuries are uncommon, constituting around 28% of cases. Typical mechanisms include posterolateral forces to the anteromedial tibia, knee hyperextension, or external tibial rotation with partial flexion. Common causes are athletic trauma, motor vehicle accidents, or falls.
Neurovascular structures may be affected. The peroneal nerve is involved in 13–17% of cases, usually from traction during hyperextension or varus stress, and less often from hematoma compression. Vascular injury, particularly to the lateral inferior genicular artery, is rare but should be considered.
2. Anatomy
Primary Static Stabilizers
The PLC’s main static stabilizers include:
Fibular Collateral Ligament (FCL): Originates proximal and posterior to the lateral femoral epicondyle, inserting on the fibular head. Primary varus stabilizer, secondary restraint to tibial rotation.
Popliteus Tendon (PT): Originates anterior to FCL on the lateral femoral condyle and inserts on the posteromedial tibia. Acts as a dynamic stabilizer against external rotation and secondary varus stress.
Popliteofibular Ligament (PFL): Arises from the popliteus musculotendinous junction, inserts on the fibular styloid. Provides secondary resistance to varus and rotational forces.(Figure-1)
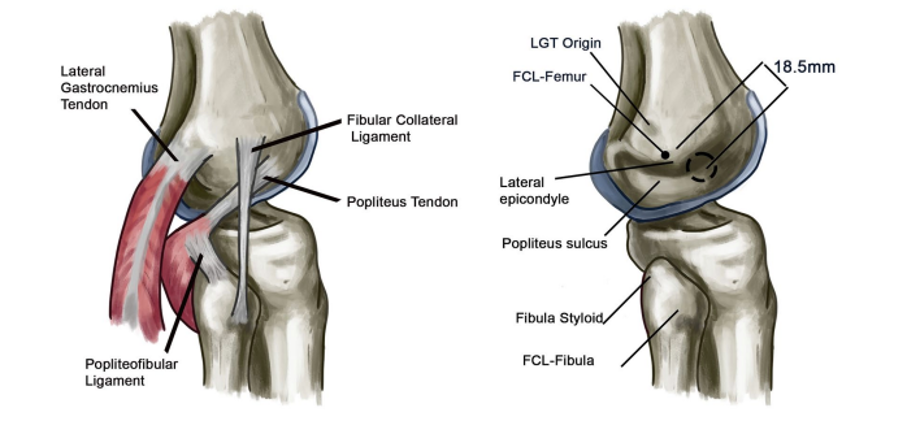
Fig-1 Posterolateral corner anatomy
Note: LGT (lateral gastrocnemius tendon), FCL (fibular collateral ligament)
Figure Reference
Source: Figueroa F, Figueroa D, Putnis S, Guiloff R, Caro P, Espregueira-Mendes J. Posterolateral corner knee injuries: a narrative review. EFORT Open Rev. 2021;6(8):676-685. Published 2021 Aug 10. doi:10.1302/2058-5241.6.200096
Reproduced from LaPrade RF, Ly TV, Wentorf FA, Engebretsen L. The posterolateral attachments of the knee: a qualitative and quantitative morphologic analysis of the fibular collateral ligament, popliteus tendon, popliteofibular ligament, and lateral gastrocnemius tendon. Am J Sports Med 2003;31:854–860.
Other Static Stabilizers
Include lateral capsule thickenings, meniscotibial and meniscofemoral ligaments, fabellofibular ligament, and arcuate ligament. Avulsion of the fibular styloid is termed an arcuate fracture.
Dynamic Stabilizers
The lateral gastrocnemius head, iliotibial band, and biceps femoris provide dynamic posterolateral stability.
Function
The PLC works synergistically with the PCL to control external tibial rotation, varus stress, and posterior translation, especially in knee flexion.
1. Clinical Presentation
Symptoms
Acute PLC injuries present with pain, swelling, and limited weightbearing. Chronic cases may show varus alignment, varus thrust gait, or posterior sag if the PCL is involved.
Physical Examination
Tests include:
Varus Stress Test: 0° flexion → combined PLC + cruciate injury; 30° flexion → isolated FCL. Graded by side-to-side displacement.
Hughston’s External Rotation Recurvatum Test: Increased hyperextension compared to the opposite side suggests PLC disruption.
Dial Test: 10–15° external rotation at 30° indicates isolated PLC; rotation at 90° indicates combined PCL + PLC injury.
2. Classification
PLC injuries are classified either by the extent of damage to the lateral structures or by the degree of rotatory instability.
Hughston Classification
Grade I: Mild tear, no abnormal motion.
Grade II: Partial tear, moderate instability.
Grade III: Complete tear, marked instability.
Fanelli and Larson Classification
Type A: PFL + PT injury → external rotation only.
Type B: PFL + PT + FCL → varus instability + external rotation.
Type C: Complete PLC disruption with cruciate injuries → severe varus and rotational instability.
3. Imaging
Radiographs
AP and lateral views detect fractures and joint congruence. Long-leg standing films assess malalignment.
MRI
Essential for acute/subacute injuries; sensitivity decreases in chronic cases (26% after 12 weeks). Coronal oblique T2 sequences best visualize PLC structures.
Stress Radiographs
Varus stress radiographs bilateral varus stress XR in 20° flexion side-to-side gap difference 2.7-4 mm indicated isolated LCL tear and side-to-side gap diffrence >4 mm indicate a grade III PLC injury.
Kneeling PCL stress views help differentiate isolated PCL vs. combined PCL + PLC injuries.
1. Treatment
Non-Operative Management
Indicated for isolated Grade I or midsubstance Grade II injuries. Protocol:
Knee immobilization in full extension for 4 weeks.
Progressive quadriceps-focused rehabilitation.
Return to sports around 8 weeks.
Operative Management
Repair
For acute avulsion injuries (FCL, PT, PFL) where anatomic reattachment is possible. Midsubstance repairs have up to 40% failure. Screws or suture anchors are used for fixation.
Reconstruction
Indicated for Grade III injuries, chronic cases, or poor tissue quality. Techniques:
Fibular-based (Larson) graft.
Trans-tibial double-bundle reconstruction.
LaPrade anatomic reconstruction (two grafts: FCL + PFL, PT).
Chronic varus malalignment may require valgus high tibial osteotomy.
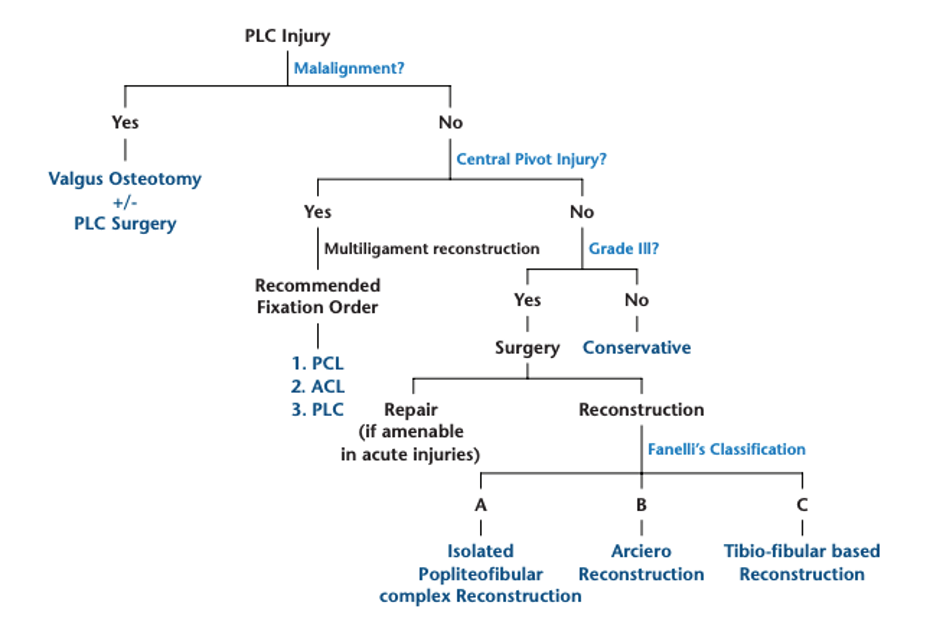
Figure-2 Surgeon based decision algorithm
Figure Reference
* Weiler A, Frosch KH, Gwinner C, Strobel MJ, Lobenhoffer P. The Posterolateral Instability Score (PoLIS) of the knee joint: a guideline for standardized documentation, classification, and surgical decision-making. Knee Surg Sports Traumatol Arthrosc. 2021;29(3):889-899. doi:10.1007/s00167-020-06044-y
1. Rehabilitation
Non-weightbearing for 6 weeks in a hinged brace.
Early passive ROM (0–90°) starting immediately or after 2 weeks.
Delayed active hamstring exercises to protect PLC.
Gradual weightbearing and closed-chain strengthening; return to sport at 6–9 months.
2. Outcomes and Complications
Anatomic reconstruction shows better stability, lower failure (6–9%) versus repair (37–40%), and superior functional scores.
Combined ACL + PLC reconstruction: higher success (88% IKDC A/B) than repair (33%).
Early surgery (<4 weeks) and correction of varus alignment improve graft survival.
Complications: arthrofibrosis, missed PLC injuries, peroneal nerve injury (15–29%).
References
Figueroa F et al., EFORT Open Rev. 2021;6:676–685. doi:10.1302/2058-5241.6.200096
LaPrade RF et al., Am J Sports Med. 2003;31:854–860.
Weiler A et al., Knee Surg Sports Traumatol Arthrosc. 2021;29:889–899. doi:10.1007/s00167-020-06044-y
Toyooka S, Persson A, LaPrade RF, Engebretsen L, Moatshe G. Injury Patterns in Posterolateral Corner Knee Injury. Orthop J Sports M 2023;11(8):23259671231184468. Published 2023 Aug 29. doi:10.1177/23259671231184468