1. Anatomy and Biomechanics
The posteromedial corner (PMC) of the knee is a complex structure that provides stability against valgus and rotatory forces. It consists of five primary components:
Superficial medial collateral ligament (MCL) – the main medial stabilizer
Deep MCL
Posterior oblique ligament (POL)
Oblique popliteal ligament
Posterior horn of the medial meniscus
The superficial MCL averages 10–12 cm in length and has two tibial insertions: proximal (1 cm below the joint line) and distal (6 cm below). The POL originates from the semimembranosus tendon and acts as a key stabilizer for internal rotation and valgus stress in extension.
Biomechanically, the proximal superficial MCL provides valgus stability throughout knee flexion, whereas the POL contributes primarily to internal rotational control near full extension. Injury to these structures can increase load on the ACL and PCL grafts, leading to graft failure if left untreated.
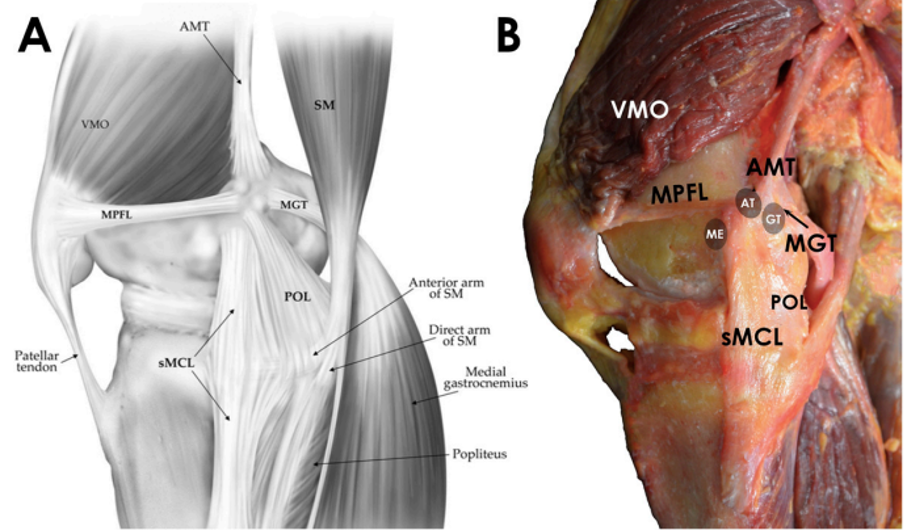
Figs. 1-A and 1-B The posteromedial corner. AMT: adductor magnus tendon, VMO: vastus medialis obliquus muscle, SM: semimembranosus muscle, MPFL : medial patellofemoral ligament, MGT: medial gastrocnemius tendon, POL: posterior oblique ligament, sMCL: superficial medial collateral ligament, ME: medial epicondyle, AT:adductor tubercle, and GT: gastrocnemius tendon. Fig. 1-B Cadaveric specimen showing soft-tissue attachments of the posteromedial side of the knee.
Figure Reference
* Cinque ME, Chahla J, Kruckeberg BM, DePhillipo NN, Moatshe G, LaPrade RF. Posteromedial Corner Knee Injuries: Diagnosis, Management, and Outcomes: A Critical Analysis Review. JBJS Rev. 2017;5(11):e4. doi:10.2106/JBJS.RVW.17.00004
2. Mechanism and Clinical Presentation
PMC injuries typically result from valgus and external rotation forces, often during sports or trauma. Patients present with medial knee pain, swelling, and instability. High-grade (Grade III) medial injuries are associated with cruciate ligament tears in up to 78% of cases.
3. Physical Examination
A detailed physical examination at varying degrees of flexion is essential:
Valgus stress test: At 20–30° flexion, gapping suggests superficial MCL injury; gapping in full extension implies POL or deep MCL involvement.
Anteromedial drawer test: Detects anteromedial rotatory instability.
Dial test: Differentiates medial vs. lateral corner injuries.
Increased valgus gapping in extension or increased internal rotation near full extension suggests combined PMC injury.
4. Imaging
Valgus stress radiographs quantify medial joint opening:
3.2 mm side-to-side difference → isolated superficial MCL tear
≥9.8 mm difference → complete PMC injury
MRI has about 87% accuracy in identifying medial-sided injuries and often shows lateral compartment bone bruising as a secondary sign. Chronic injuries may reveal Pellegrini-Stieda calcification.
5. Classification
The AMA grading system classifies medial injuries as:
Grade I: 0–5 mm gapping (pain, no instability)
Grade II: 6–10 mm gapping with firm endpoint
Grade III: >10 mm gapping with no endpoint
6. Treatment Principles
Nonoperative management is recommended for Grade I–II and isolated Grade III superficial MCL injuries. Treatment includes bracing for 5–7 weeks, quadriceps strengthening, and gradual range-of-motion exercises. Proximal MCL tears heal better than distal ones due to superior vascularity.
Operative management is indicated for:
Grade III injuries with valgus gapping in extension
Combined ligamentous injuries (e.g., with ACL or PCL tears)
Chronic valgus and rotatory instability
7. Surgical Techniques
The PMC reconstruction aims to anatomically restore the proximal and distal divisions of the superficial MCL and the posterior oblique ligament (POL) using two separate grafts. Through an anteromedial incision, the sartorial fascia is opened to expose the semitendinosus, gracilis, and semimembranosus tendons. Tibial tunnels are prepared first for the distal MCL and then for the POL anterior to the semimembranosus. Femoral tunnels are made just anterior to the medial epicondyle for the MCL and near the gastrocnemius tubercle for the POL. After femoral fixation, the POL is tensioned in extension, and the MCL is secured at 20° flexion in neutral rotation with slight varus stress to restore stability.
Single-stage reconstruction is preferred in multiligament injuries to reduce graft stress and allow early rehabilitation.
8. Postoperative Rehabilitation
Early protected range of motion (0–90° for 6 weeks), partial weight-bearing, and hinged bracing are recommended. Full return to sport usually occurs at 6–9 months if strength and stability criteria are met.
9. Complications
Common complications include arthrofibrosis, stiffness, and infection. Early, aggressive rehabilitation is key to preventing stiffness.
10. Key Takeaways
The PMC plays a vital role in valgus and rotational stability.
Accurate diagnosis requires understanding anatomy, biomechanics, and imaging interpretation.
Anatomic reconstruction of the MCL and POL provides superior biomechanical and clinical outcomes.
Early recognition and management are essential to protect cruciate grafts and restore stable knee function.
References
Cinque ME, Chahla J, Kruckeberg BM, DePhillipo NN, Moatshe G, LaPrade RF. Posteromedial Corner Knee Injuries: Diagnosis, Management, and Outcomes: A Critical Analysis Review. JBJS Rev. 2017;5(11):e4. doi:10.2106/JBJS.RVW.17.00004
Madi S, Acharya K, Pandey V. Current concepts on management of medial and posteromedial knee injuries. J Clin Orthop Trauma. 2022;27:101807. Published 2022 Feb 18. doi:10.1016/j.jcot.2022.101807
3. Fusco S, Albano D, Gitto S, Serpi F, Messina C, Sconfienza LM. Posteromedial Corner Injuries of the Knee: Imaging Findings. Semin Musculoskelet Radiol. 2024;28(3):318-326. doi:10.1055/s-0044-1779718