Figures

Deformity in the context of the lower limb is defined as an abnormality in the normal geometry and morphology of the skeletal structure. Human lower limbs are specifically adapted for efficient bipedal gait, and deviations from this consistent morphology—whether following injury or resulting from developmental irregularities—constitute a deformity. A bone deformity can be fully characterized by six parameters: three rotations (angulation and torsion) and three projected displacements (translation and length). These abnormalities are generally categorized into three origins: congenital , which occur due to in utero dysplasia; developmental, which are progressive during childhood due to differential growth; and acquired , which typically stem from trauma or surgery.
Understanding the clinical and radiographic "personality" of a deformity is fundamental for management planning. Significant deviations from normal alignment patterns result in uneven joint loading, which increases contact stress and leads to accelerated cartilage damage and degenerative arthrosis. Symptoms such as pain, abnormal walking patterns, and concerns about appearance often drive patients to seek treatment. Modern deformity analysis combines comprehensive clinical assessment with sophisticated radiological imaging and geometric principles to plan accurate surgical corrections, often utilizing specialized software to map deformities in three-dimensional space.
Deformity Evaluation
Clinical evaluation is the fundamental precursor to managing skeletal deformity, providing a "personality" to the abnormality that radiographic analysis cannot offer in isolation,. A comprehensive summary of clinical evaluation includes the following key components:
1. Detailed Clinical History
The history must differentiate between congenital, developmental, and acquired (post-traumatic) origins, as these dictate different management strategies,.
Congenital/Developmental: Evaluation includes prenatal events (maternal illness, drug exposure), family history, and recording motor milestones such as head control, pulling to stand, and walking,,.
Post-Traumatic: Assessment requires a surgical timeline of previous procedures, specifications of existing implants, and focused history regarding past infections (wound healing, antibiotic use, or sinus formation),.
Symptomatic Profile: Quantify the effects of the deformity on function and lifestyle, specifically addressing pain, abnormalities in walking patterns, and concerns about aesthetic appearance.
2. Gait Assessment
Formal gait assessment involves repeated observation of the patient walking for a distance sufficient to establish a consistent pattern.
Panoramic View: Evaluation should occur from the front, side, and back in the frontal, lateral, and axial planes.
Observation Goals: Clinicians must discriminate between gait abnormalities caused by pain (antalgic), skeletal geometry (short leg or hiking), joint instability (varus/valgus thrust), or contractures.
3. Physical Examination of Segments and Joints
The examination should move systematically through skeletal proportions, limb rotation, and limb-length discrepancy.
Joint Assessment: Every joint adjacent to the deformity must be checked for active and passive range of motion, pain, and ligament laxity,. Identifying fixed flexion deformities (FFD) or hyperextension (HE) is critical to prevent loss of function after surgical correction,.
Limb Length: Measurement of the total length from the sole of the foot to the pelvic brim determines shortening,. Clinicians distinguish between "true" (skeletal) and "apparent" length differences,.
Torsional Profile: This clinical exercise describes axial angulation (torsion) and joint movement (rotation). It typically involves assessing hip rotation in the prone or supine position and measuring the thigh-foot axis or transmalleolar axis,.
4. Soft-Tissue Envelope and Neurovascular Status
The condition of non-skeletal tissues fundamentally affects surgical options and outcomes.
Soft-Tissue Envelope: Comprehensive assessment identifies skin grafts, tethering, or scars that may preclude certain osteotomy sites or internal fixation.
Neurovascular Status: Individual peripheral nerves must be tested for motor and sensory function, and arterial pulses should be verified, using a Doppler probe if necessary. Clinicians should also look for signs of previous compartment syndrome, such as uncompliant fibrotic muscle, which increases the risk of joint contractures during lengthening.
5. Defining Treatment Goals
The clinical evaluation concludes by identifying achievable goals understood by the patient and surgeon, such as eradicating pain, producing a plantigrade foot, or enabling the use of off-the-shelf footwear,. Evaluation is an ongoing process, as an evolving loss of joint range during treatment is a compelling reason to alter surgical plans.
Deformity Analysis
Lower-limb deformity analysis requires a systematic integration of clinical findings, standardized radiological imaging, and geometric principles to accurately define the abnormality and plan correction. For the radiological analysis the following components are essential:
1. Standardized Radiological Imaging
Radiographs provide the geometric data necessary for planning. Requirements include:
Weight-Bearing Views: Full-length, standing antero-posterior (AP) and lateral radiographs from the hip to the ankle.
Magnification Control: The use of a radio-opaque scalar (scalar ball) of known dimensions to correct for magnification errors, which is critical for accurate distance measurements.
Proper Positioning: Ensuring the patella is facing forward to avoid parallax and projection errors during axis construction.
Advanced Imaging: CT scans may be required for precise assessment of complex torsional deformities.
2. Geometric Analysis Parameters
To fully characterize a deformity, a clinician must define six parameters: rotations (angulation/torsion) and translations (displacement/length) in three planes. Key steps include:
Identification of Joint Centers: Locating the centers of the hip, knee, and ankle. Draw joint orientation lines.
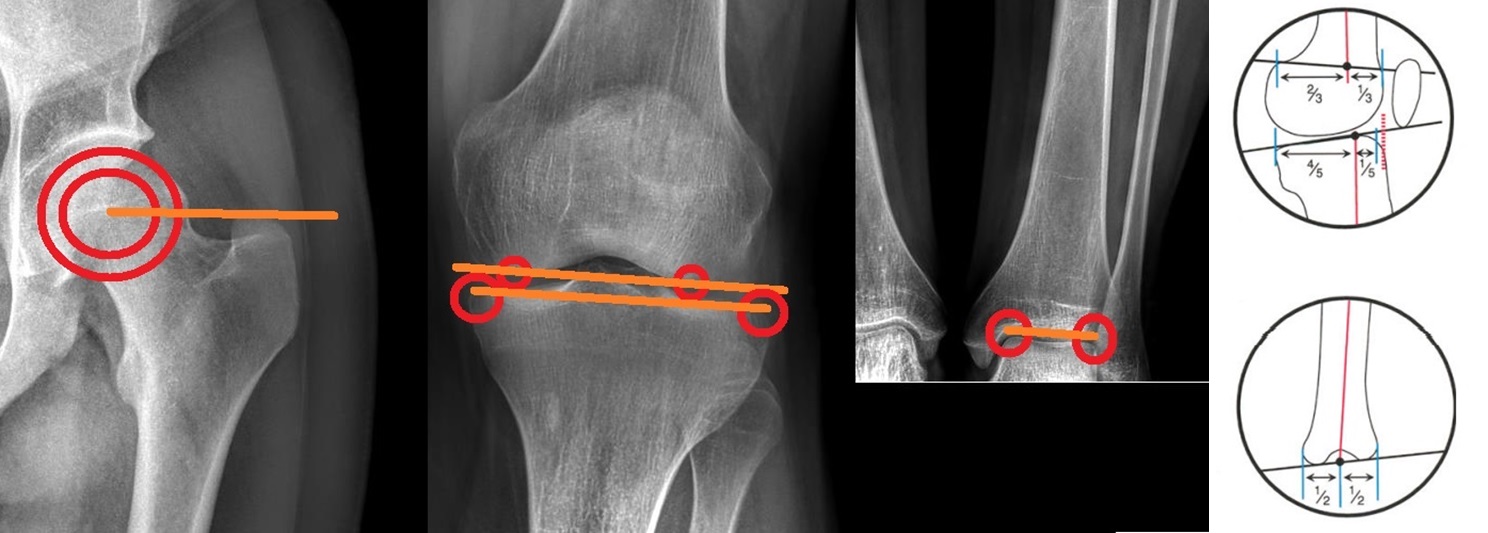
Mechanical and Anatomical Axes: Drawing the axes for the whole limb and individual bone segments. Mechanical axes are connecting center of joints.
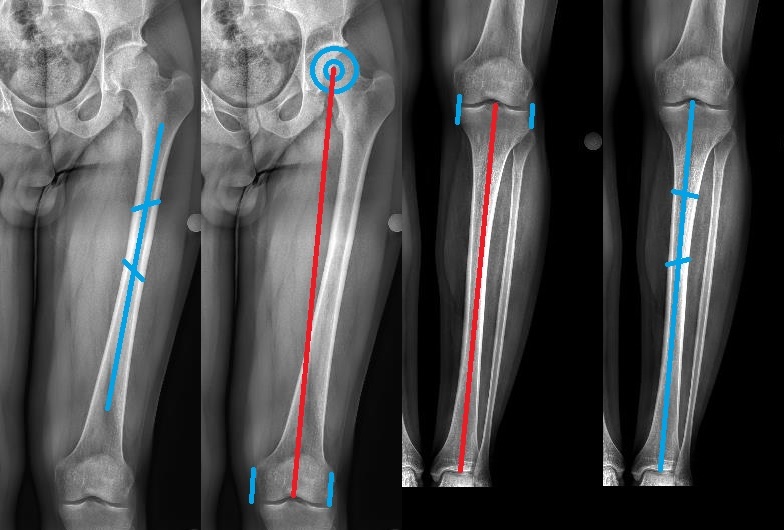
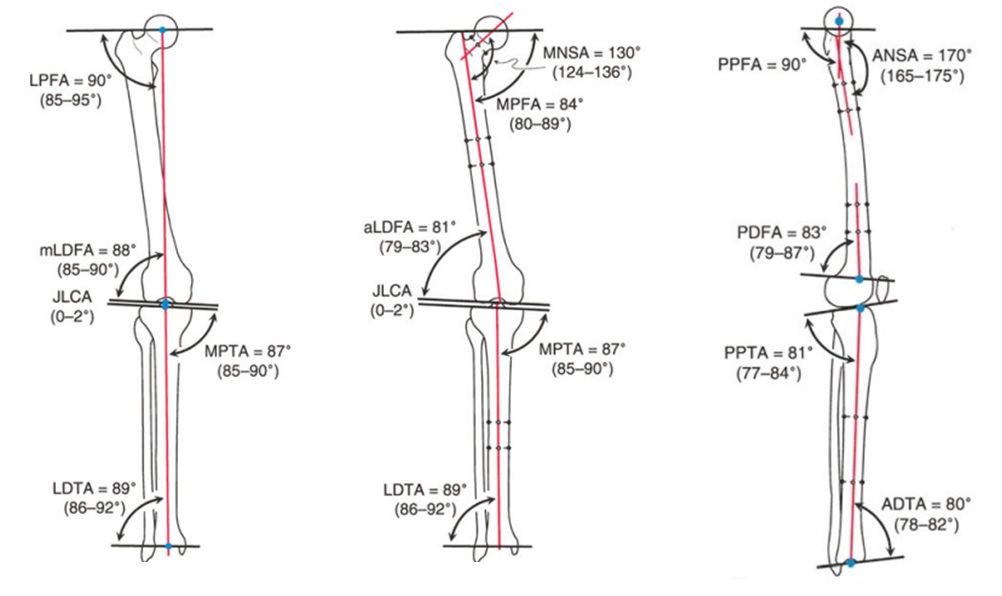
Joint Orientation Angles: Measuring standard angles (e.g., mLDFA, MPTA, LDTA) and comparing them to population normals or the contralateral "normal" limb.
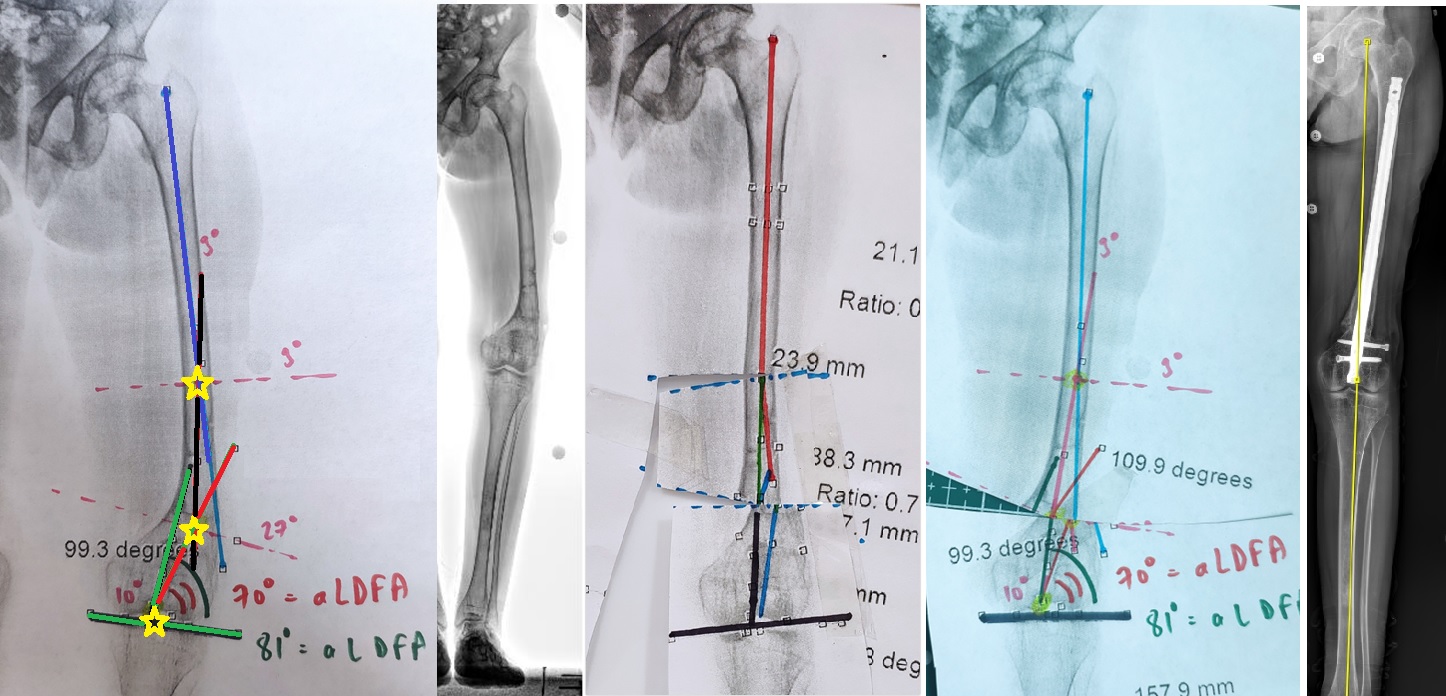
CORA (Center of Rotation of Angulation): Determining the exact point where the proximal and distal axes intersect to locate the apex of the deformity.
4. Planning Tools and Techniques
Analysis can be performed using traditional or digital methods:
Manual Tools: Pencil, protractor, ruler, and tracing paper used directly on radiographic films to simulate osteotomies and corrections.
Software Applications: Specialized programs such as TraumaCad®, OrthoView™, Click2Correct®, Bone Ninja for rapid and detailed digital analysis.
Oblique Plane Analysis: Since deformities often exist in an oblique plane, mathematical trigonometric formulas or graphic methods are used to calculate the true magnitude and direction from bi-planar (AP and lateral) data.
Mounting Parameters: For hexapod fixators, specific "mounting parameters" (offsets of the ring relative to the bone's origin) must be defined.
References
1- Monsell, F. (2022). Fundamentals of Lower-Limb Deformity Analysis. In Fundamentals of Lower-Limb Deformity Analysis. NPM Publishing Ltd Shropshire, UK.
2- Paley, D. (2014). Principles of deformity correction. Springer.
3- Standard, S. C., Herzenberg, J. E., Conway, J. D., Siddiqui, N. A., McClure, P. K., & Assayag, M. J. (2021). The art of limb alignment. Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore.