Figures
In the context of lower-limb deformity correction, an osteotomy is the surgical division of a bone to realign its axes and restore normal geometry. The success of an osteotomy depends on the systematic integration of geometric principles, biological factors, and appropriate hardware selection.
1. The Three Geometric Variables
The relationship between three specific points determines the final alignment and morphology of the bone:
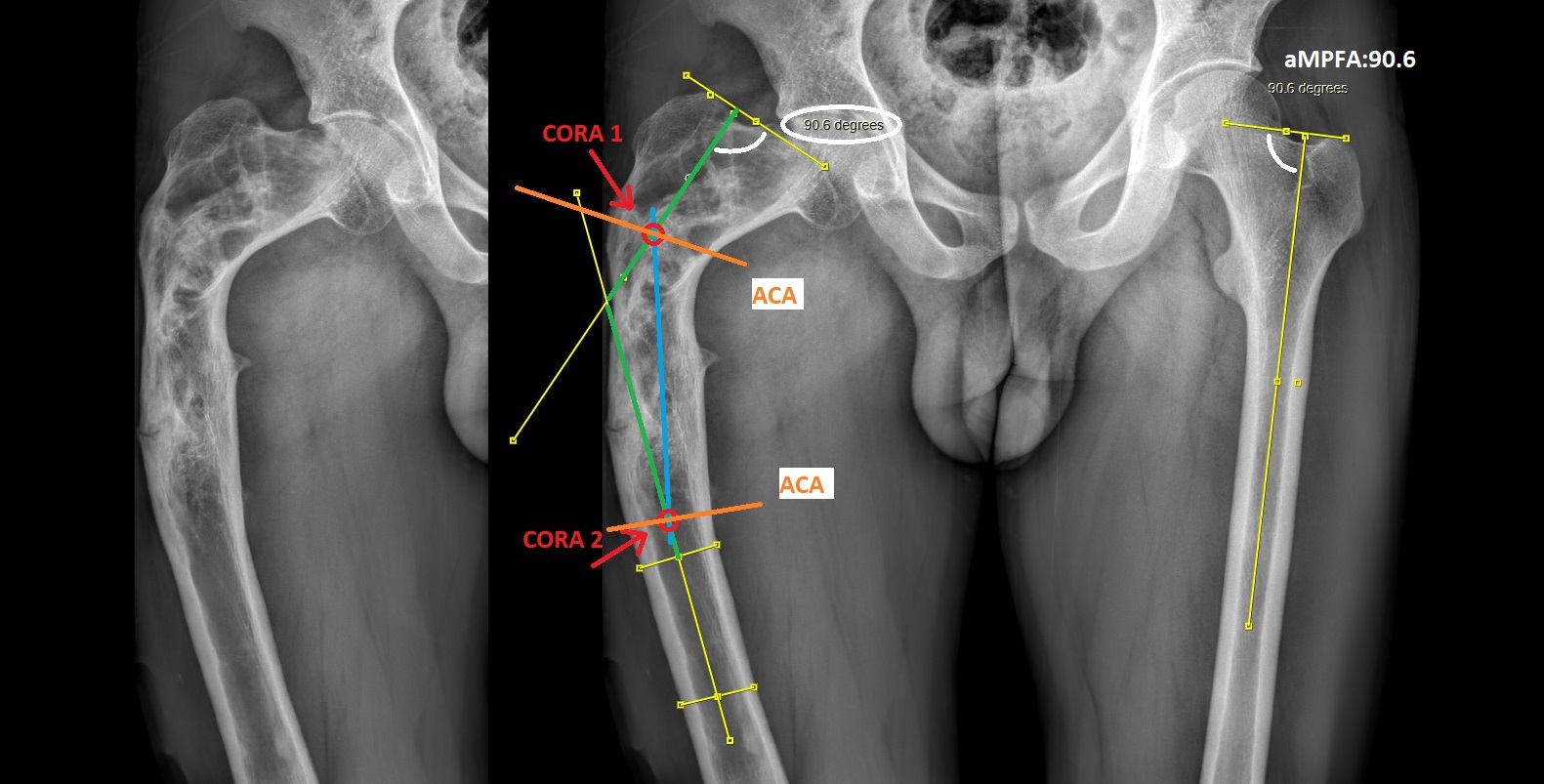
CORA (Center of Rotation of Angulation): The intersection point of the proximal and distal axis lines of a deformed bone.
ACA (Angulation Correction Axis): The imaginary line in space around which the bone segments are rotated during correction.
Osteotomy Level: The actual site where the bone is surgically cut.
2. Paley’s Osteotomy Rules
These rules dictate whether a correction will result in pure angulation or obligatory translation:
Rule 1: If the osteotomy and the ACA both pass through the CORA, the bone segments will angulate without any translation (displacement). The axes will become perfectly collinear.
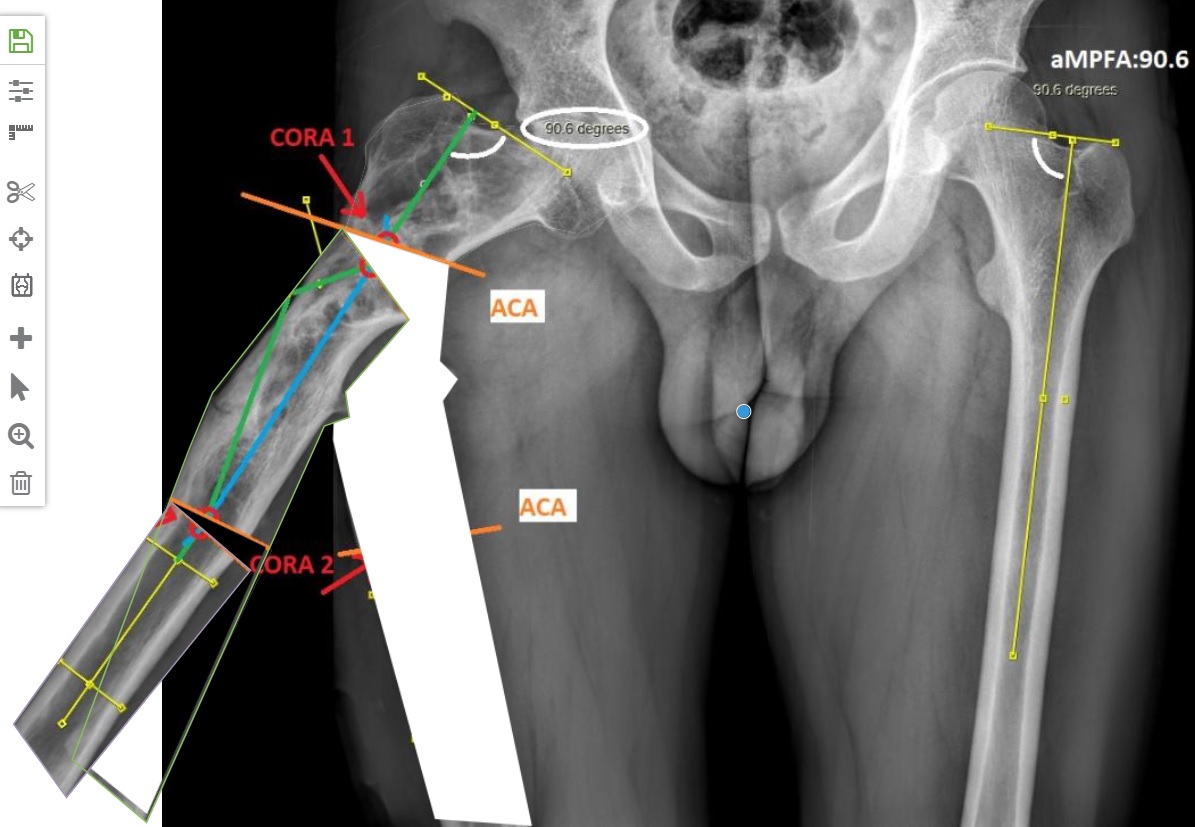
Rule 2: If the ACA passes through the CORA but the osteotomy is at a different level, the bone ends will both angulate and translate relative to each other. However, the proximal and distal axes will still achieve perfect collinear alignment.
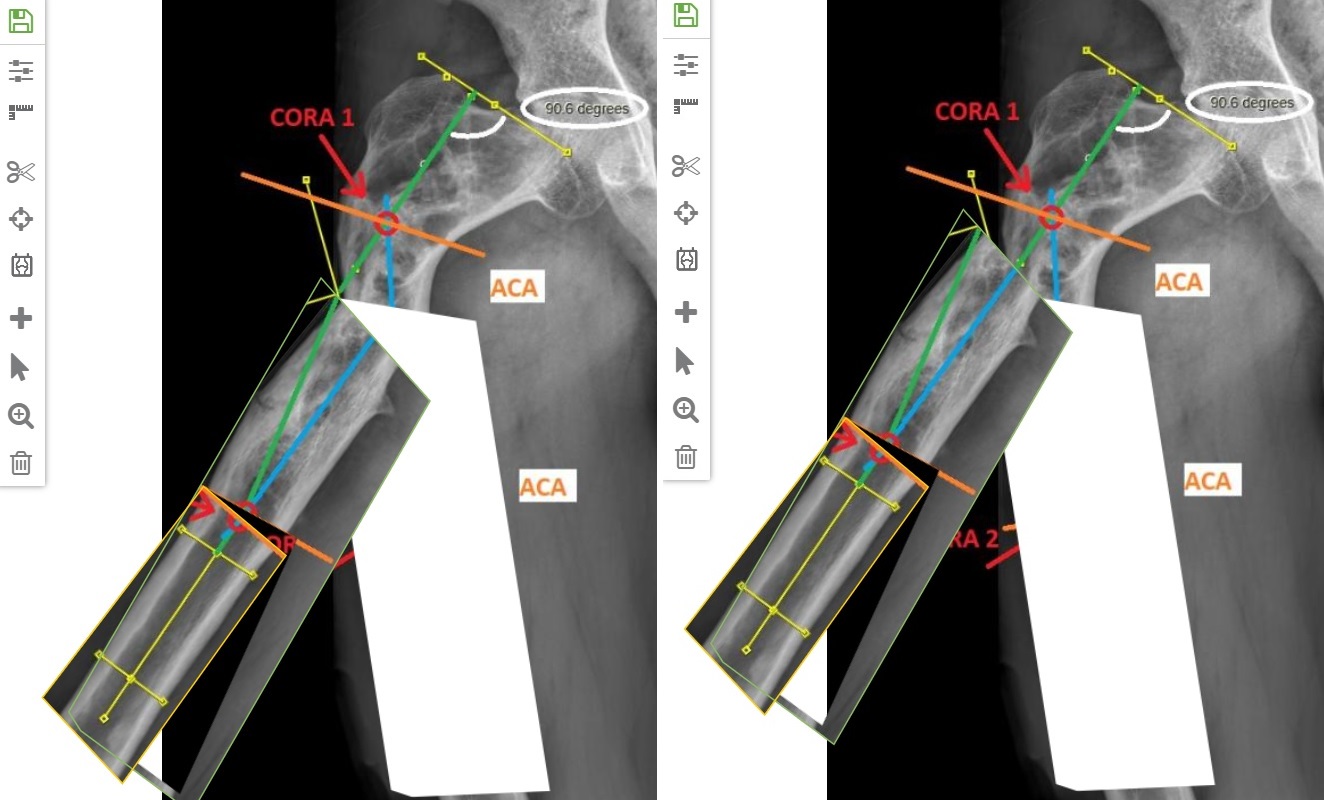
Rule 3: If the ACA does not pass through the CORA, the axes will remain parallel but translated (not collinear) after correction, resulting in a secondary deformity.
3. Basic Osteotomy Types
Opening Wedge: Performed by cutting the bone and rotating it around an ACA on the convex cortex. This adds length but requires bone graft or gradual distraction to fill the gap.
Closing Wedge: Performed by removing a wedge of bone with the ACA on the concave cortex. This provides excellent stability and bone contact but results in limb shortening.
Neutral (Hemi-wedge): A combination where a half-wedge is removed from one side and used as a graft on the other, maintaining the original bone length.
Dome (Cylindrical) Osteotomy: A circular cut that allows rotation. A Focal Dome is centered exactly on the CORA, following Osteotomy Rule 2 to ensure axis realignment while maintaining maximum bone contact.
4. Surgical and Biological Principles
Soft Tissue Integrity: Low-energy (percutaneous) techniques using multiple drill holes or Gigli saws are preferred to preserve the periosteum and blood supply, enhancing healing.
Thermal Protection: When using motorized saws, constant irrigation with cold saline and a "stop-start" technique are critical to prevent thermal necrosis of the bone.
Order of Correction: In acute corrections, translation and rotation should precede angulation. Angulating first creates soft tissue tension that can "lock" the bone ends and prevent necessary translation.
Hardware Selection: The choice between plates, intramedullary nails, or external fixators depends on the patient's age, bone quality, and whether the correction is acute or gradual.