Figures
Definition
Distal tibial osteotomy (DTO), commonly referred to as supramalleolar osteotomy (SMO), is a joint-preserving realignment procedure performed proximal to the ankle joint to correct coronal plane malalignment and redistribute tibiotalar load.
Core Concept
Malalignment → asymmetric tibiotalar loading → cartilage degeneration
SMO → mechanical axis correction → load shift to preserved cartilage
Primary goal:
Restore neutral tibiotalar congruency
Unload the degenerative compartment
Most common indication:
Post-traumatic ankle osteoarthritis (~78%)
Indications
Primary
Varus or valgus ankle OA with extra-articular deformity (supramalleolar origin)
Takakura stage 1–3a (selected 3b cases possible)
Age <60, active patient
Preserved ankle ROM (≥10° dorsiflexion)
Talar tilt <10°
Failed conservative treatment
Expanded / Functional Indications
Post-traumatic ankle arthritis (most common)
Malunited distal tibia/fibula fractures
Early joint incongruity with preserved cartilage
Contraindications
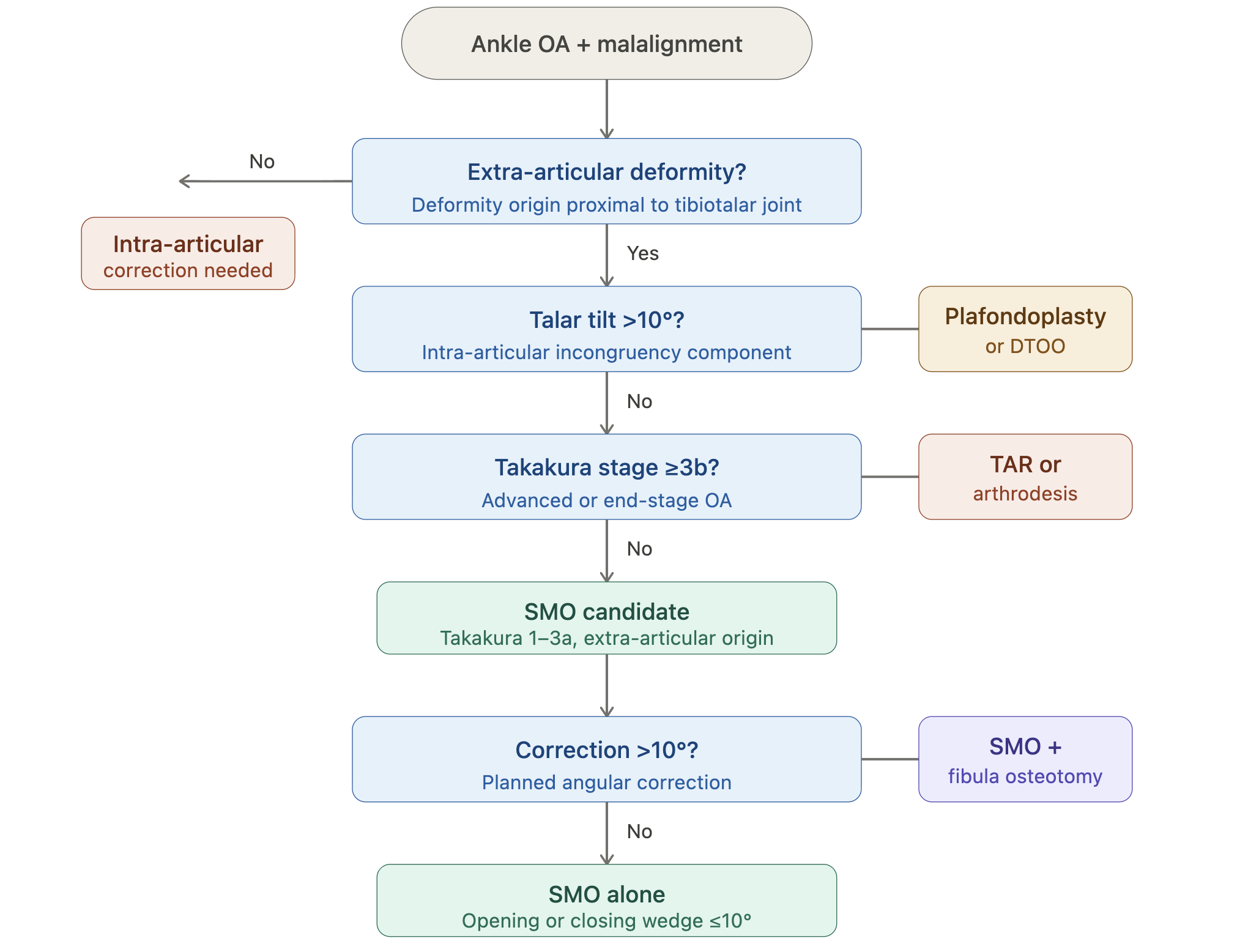
Advanced OA (Takakura 3b–4) → consider arthrodesis or TAR
Talar tilt >10° with intra-articular deformity
Inflammatory arthritis
Severe osteoporosis
Fixed hindfoot deformity
Active infection
Deformity Assessment
CORA (center of rotation of angulation)
Talar tilt
TAS angle (target: 90–95°)
Hindfoot alignment
Subtalar joint status
Key principle:
Correction must be performed at the true deformity origin
Surgical Techniques
1. Medial Opening Wedge
Best for:
Varus deformity <10°
Early OA
Pros:
Precise correction
No fibula osteotomy (often)
Cons:
Requires bone graft
Risk of delayed union
2. Lateral Closing Wedge
Best for:
Varus deformity
Larger corrections
Pros:
Faster healing
No graft required
Cons:
Requires fibula osteotomy
Less adjustable
3. Dome (Rotational) Osteotomy
Best for:
Multiplanar deformities
Talar tilt >4°
Key feature:
Allows 3D correction
Technically demanding
4. DTOO (Oblique Osteotomy — Teramoto)
Best for:
Advanced varus OA
Incongruent joints
Key feature:
Oblique cut (proximal-medial → distal-lateral)
No fibula osteotomy required
Fibula Factor (High-Yield)
Without fibula osteotomy → correction ≈ ~10°
With fibula osteotomy → correction ≈ ~19–20°
Rule:
Correction >10° → fibula osteotomy required
Outcomes
Clinical
VAS: 7.0 → ~2.5
AOFAS: ~52–57 → ~78–83
Patient satisfaction: ~89%
Radiological
TAS restored to 90–95°
Improved talar alignment
Survivorship / Failure
Failure rate: ~3.7–6.8%
Complication rate: ~5–10%
Reoperation rate: ~28%
Most reoperations = hardware removal (not failure)
Complications
Nonunion (~1.6%)
Delayed union
Superficial infection
Loss of correction
Residual deformity
Decision Algorithm
Pearls & Pitfalls
Pearls
Always identify CORA before planning
Evaluate subtalar joint mobility
Counsel patients: reoperation ≠ failure
Consider entire lower limb alignment (knee + ankle)
Pitfalls (High-Yield)
Performing correction at wrong level → secondary deformity
Ignoring talar tilt → residual joint incongruity
Missing subtalar pathology → incomplete correction
Using SMO in Takakura 3b–4 → poor outcomes
Forgetting fibula osteotomy in large corrections
Assuming reoperation = failure (mostly hardware removal)
Overlooking kinetic chain (HTO affects ankle alignment)
Ideal Patient Profile
Age <60 · Active · Takakura 1–3a · ROM ≥10° · Extra-articular deformity · Preserved opposite compartment
Clinical Insight
SMO is not simply an osteotomy—it is a joint-preserving alignment strategy. Its success depends on accurate deformity localization, proper indication, and understanding of ankle–hindfoot biomechanics.
Bottom Line
SMO/DTO is an effective bridge procedure that delays the need for arthrodesis or total ankle replacement in young, active patients with post-traumatic ankle OA.
Strong mid-term outcomes
High satisfaction
But notable reoperation rate
Know the stage, measure the tilt, respect the fibula.
References
Harnroongroj, T., & Chuckpaiwong, B. (2017). Benefit of Adding Fibular Osteotomy to Open-Wedge, Valgus, Distal Tibial Osteotomy for Correcting Varus Ankle Arthritis: An In Vitro Study. The Journal of Foot & Ankle Surgery, 56, 234–237.
Aujla, R. S., Perianayagam, G., Siddiqui, B. M., Divall, P., & Bhatia, M. (2021). Distal tibial osteotomy for varus ankle arthritis: A meta-analysis and systematic review. Journal of Arthroscopy and Joint Surgery, 8, 238-245.
Teramoto, T., Harada, S., Takaki, M., et al. (2018). The Teramoto distal tibial oblique osteotomy (DTOO): surgical technique and applicability for ankle osteoarthritis with varus deformity. Strategies in Trauma and Limb Reconstruction, 13, 43–49.
Zhao, Y. Q., Wang, X. W., Li, H., Gong, X. F., & Wu, Y. (2025). Supramalleolar osteotomy outcomes for post-traumatic fracture-related ankle arthritis: a retrospective analysis. BMC Surgery, 25(366).
Butler, J. J., Azam, M. T., Weiss, M. B., Kennedy, J. G., & Walls, R. J. (2023). Supramalleolar osteotomy for the treatment of ankle osteoarthritis leads to favourable outcomes and low complication rates at mid-term follow-up: a systematic review. Knee Surgery, Sports Traumatology, Arthroscopy, 31, 701–715.
Oktem, U., Dastan, M. C., Avci, H., et al. (2026). High Tibial Osteotomy Is Associated with Improvements in Both Knee and Ankle Alignment in Medial Compartment Osteoarthritis. Journal of Clinical Medicine.
Xue, W., Chen, T., Wahafu, P., et al. (2022). Efficacy evaluation and systematic review of supramalleolar osteotomy for treatment of varus-type ankle arthritis. Journal of Orthopaedic Surgery, 30(2), 1–10.